Pablo Alcántara Costas Martingano 1, 2, Tomás Vanegas 1, 2, Paul Vargas Mieles 1, 2, Nicolás Silva Croome 1, Ezequiel Besmalinovich 1, 2, Guillermina Sorasio 2, 3 MTSAC, Nicolás Caruso 2, 3 MTSAC, Adrián Lescano1, 2, 3, 4, 5, MTSAC
1 Department of Cardiology. Sanatorio de la Trinidad Quilmes. Buenos Aires
2 Department of Cardiology. Centro Gallego de Buenos Aires. Autonomous City of Buenos Aires
3 Pulmonary hypertension Team Sanatorio de la Trinidad Ramos Mejía. Buenos Aires
4 Pulmonary hypertension Team Sanatorio de la Trinidad Ramos Mejía. Buenos Aires
5 Pulmonary hypertension Team Sanatorio Mater Dei. Autonomous City of Buenos Aires
Address for reprints: Nicolás Caruso. E-mail: niccaruso@hotmail.com
Rev Argent Cardiol 2024;92:xxx-xxx. http://dx.doi.org/10.7775/rac.v92.i2.20745
ABSTRACT
Background: Pulmonary hypertension (PH) is associated with high morbidity and mortality and its prognosis is determined by the right ventricular function and right ventricular-pulmonary artery coupling. Several hemodynamic parameters have been proposed to better characterize the risk for adverse disease progression.
Objective: The aim of this study was to determine the predictive ability of various hemodynamic parameters that can be calculated during RHC to predict serious events.
Methods: In this retrospective multicenter and descriptive cohort study of patients with PH, hemodynamic variables values were divided as high or low risk based on the 2022 European guidelines, or mean or median values in our population.
Results: A total of 324 patients with PH were included; mean age was 61.5 years and 69% were women; 62.1 % of the patients were in Group 1 and 19.2 % in Group 3. In a median (IQR) follow-up of 23(14-44) months, the event rate (death or hospitalization for heart failure) was 60.6% and all-cause mortality was 24.5%. The cut-off values associated with risk for the different hemodynamic variables were: cardiac index (CI) 2.72 L/min/m2, systolic volume index (SVI) 33.1 ml/m2, pulmonary vascular resistance (PVR) 6 Wood units (WU), pulmonary artery pulsatility index (PAPI) 3.76, right ventricle systolic work index (RVSWI) 11.6 g.m/m2, and pulmonary arterial compliance 1.84 mL/mm Hg. Elevated PVR was associated with a higher rate of composite events, while high-risk CI, SVI, PVR, and compliance were associated with higher mortality at follow-up.
Conclusions: While CI and SVI are adequate predictors of risk, PVR and compliance demonstrate similar or even better risk prediction in patients with PH. Additional research is necessary to validate these parameters during follow-up.
Key words: Pulmonary hypertension - Prognosis - Hemodynamics - Pulmonary vascular resistance
RESUMEN
Introducción: La hipertensión pulmonar (HP) se asocia con elevada morbimortalidad y su pronóstico está determinado por la función del ventrículo derecho y el acople ventrículo-arterial pulmonar. Diversos parámetros hemodinámicos han sido propuestos para caracterizar el riesgo de evolución adversa.
Objetivos: Determinar la capacidad de predicción de eventos graves, de diversos parámetros hemodinámicos medidos por cateterismo derecho.
Material y métodos: Estudio multicéntrico, descriptivo, de cohorte retrospectiva de pacientes con HP. Se dividió a los datos hemodinámicos en alto o bajo riesgo según lo definido por las recomendaciones europeas de 2022, o según media o mediana de nuestra población.
Resultados: Fueron incluidos 324 pacientes con HP, con edad media 61,5 años y 69% de sexo femenino; 62,1 % de los pacientes del Grupo 1 y 19,2 % del Grupo 3. La tasa de eventos (muerte o internaciones) en un seguimiento mediano de 23 (RIC 14-44) meses fue 60 % y la mortalidad global 24,5 %. Los valores de corte para definir riesgo de las diferentes variables fueron: índice cardíaco (IC) 2,72 L/min/m2, índice de volumen sistólico (IVS) 33,1 mL/lat./m2, resistencia vascular pulmonar (RVP) 6 unidades Wood (UW), índice de pulsatilidad de la arteria pulmonar (IPAP) 3,76, índice de trabajo sistólico del ventrículo derecho (ITSVD) 11,6 g.m/m2, compliance vascular pulmonar 1,84 mL/mmHg. La RVP elevada se asoció a mayor frecuencia de eventos combinados, mientras que valores de alto riesgo de IC, IVS, RVP y compliance presentaron asociación con mayor mortalidad en el seguimiento.
Conclusiones: Si bien el IC y el IVS presentaron una adecuada predicción de riesgo, variables como la RVP y la compliance mostraron similar, e incluso mejor predicción de eventos graves en HP. Se necesitan nuevos estudios que validen estos parámetros en el seguimiento.
Palabras clave: Hipertensión pulmonar - Pronóstico - Hemodinamia - Resistencia pulmonar
Received: 10/01/2023
Accepted: 12/07/2024
INTRODUCTION
Pulmonary hypertension (PH) is a multifactorial entity due to multiple causes and is defined as a complex hemodynamic condition characterized by a mean pulmonary arterial pressure (mPAP) > 20 mm Hg. Regardless of the underlying cause (such as left heart disease, respiratory disease, or pulmonary vascular disease), PH is always associated with high morbidity and mortality, and its occurrence always worsens the clinical course of patients.
Its prognosis is determined by the ability of the right ventricle (RV) to adapt to the progressive excessive pressure load of the pulmonary circulation (RV-pulmonary artery coupling). In this sense, several hemodynamic parameters have been proposed to better characterize this issue. The 2022 European Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension identify several prognostic hemodynamic parameters in patients with pulmonary arterial hypertension, including right atrial pressure (RAP), cardiac index (CI), central venous oxygen saturation (SvO2), and stroke volume index (SVI). (1, 2) These parameters have been validated during follow-up, especially CI and SvO2. (3,4)
There are other hemodynamic parameters of right ventricular function and RV-pulmonary artery coupling that can be measured during right heart catheterization (RHC). These include pulmonary vascular resistance (PVR), pulmonary arterial compliance, RV systolic work index (RVSWI) (5,6) or pulmonary artery pulsatility index (PAPI). (7,8) Although PVR is widely used as a hemodynamic parameter in pulmonary arterial hypertension (PAH) and even as a clinical endpoint in most current clinical trials, recent European recommendations do not consider it a prognostic marker. The REVEAL registry only uses a cut-off value of 5 Wood units (WU) with little hierarchy within the score based on baseline characteristics. (9) This may be due to the fact that some studies have failed to demonstrate its prognostic value. (10,11)
However, we lack information on the prognostic value of the different measurements of right ventricular function and pulmonary circulation that can be obtained in the catheterization laboratory. In this context, the aim of this study was to determine the predictive ability of various hemodynamic parameters that can be calculated during RHC to predict serious events such as death or hospitalization due to worsening pulmonary hypertension.
METHODS
The Pulmonary Hypertension Working Group consists of a multidisciplinary team working in 5 centers in the Autonomous City of Buenos Aires and the Greater Buenos Aires Area (Sanatorio de la Trinidad Quilmes, Centro Gallego de Buenos Aires, Sanatorio Dupuytren, Sanatorio Trinidad Ramos Mejía and Sanatorio Mater Dei). We performed a retrospective cohort analysis of our registry which included consecutive patients recorded in the work group database who underwent RHC between January 2011 and May 2023. All the patients signed an informed consent form to undergo RHC and authorized the anonymous use of the result of the test for research purposes. All patients with PH, defined as mPAP > 20 mmHg at rest, were included in the analysis. Patients were classified into PH groups 1 to 5 according to international recommendations. Group 1 patients with PAH were subdivided into idiopathic PAH, associated with connective tissue diseases, congenital heart disease, human immunodeficiency virus (HIV) infection or drugs, and portopulmonary hypertension, following the same recommendations.
Cardiac index was calculated according to the formula:
CI = CO / BSA
where CI: cardiac index, CO: cardiac output, BSA; body surface area
Stroke volume index was calculated according to the formula:
SVI = CI / HR
where SVI: stroke volume index, CI: cardiac index, HR: heart rate
Pulmonary vascular resistance was calculated according to the formula:
PVR = (mPAP – PAWP) / CO
where PVR: pulmonary vascular resistance, mPAP: mean pulmonary arterial pressure, PAWP: pulmonary arterial wedge pressure; CO: cardiac output
Pulmonary artery pulsatility index was calculated according to the formula:
PAPI = (sPAP – dPAP) / RAP
where PAPI: pulmonary artery pulsatility index, sPAP: systolic pulmonary artery pressure, dPAP: diastolic pulmonary artery pressure; RAP: right atrial pressure
Pulmonary arterial compliance was calculated according to the formula:
C = SV / (sPAP – dPAP)
where C: compliance, SV: stroke volume, sPAP: systolic pulmonary artery pressure, dPAP: diastolic pulmonary artery pressure
Finally, RVSWI was calculated according to the formula:
RVSWI = (mPAP – RAP) * SVI * 0.0136 where RVSWI: right ventricular systolic work index, mPAP: mean pulmonary arterial pressure, RAP: right atrial pressure, SVI: stroke volume index
The values of the hemodynamic variables were defined as high or low risk as stated by the 2022 ESC (European Society of Cardiology) recommendations. Low risk was defined as CI > 2.5 L/min/m2 and SVI > 38 mL/m2. For variables not defined by the guidelines, we used the mean or median values of our population, according to their distribution. Quantitative variables with normal distribution are expressed as mean ± standard deviation (SD) and those with non-normal distribution are expressed as median and interquartile range (IQR). The incidence of events (death, hospitalization due to worsening PH, or need for dose escalation of a specific therapy) was assessed and compared in the high-risk and low-risk groups for each variable using the chi square test and logistic regression analysis with calculation of odds of the occurrence of events (odds ratio).
RESULTS
A total of 324 patients with PH documented by RHC were prospectively included in the registry. Mean age was 61.5 ± 17.6 years and 69.0% were men. Median (IQR) follow-up was 23 (14-44) months. The patients were classified as follows: 62.1% in Group 1, 8. 7% in Group 2, 19.2% in Group 3, 7.7% in Group 4, and 2.1% in Group 5. In group 1, the etiologies were idiopathic PAH in 57.1%, associated with connective tissue diseases in 26.1%, associated with congenital heart disease in 12.8%, portopulmonary hypertension in 1.9%, associated with HIV in 1.4%, and associated with drugs in 0.4%. The event rate (death or hospitalization for heart failure) was 60.6% and all-cause mortality was 24.5%. The mean ± SD values or median (IQR) values of the hemodynamic variables of the sample were: CI 2.72 ± 0.72 L/min/m2, SVI 33.1 ± 12.4 mL/m2, PVR 6 (3.7-9.8) WU, PAPI 3.76 (2.5-5.8), RVSWI 11.6 (8.6- 16.5) g.m/m2, and pulmonary arterial compliance 1.84 (1.09-3.03) mL/mm Hg. Tables 1 and 2 show the event rates for each hemodynamic variable in the low-risk and high-risk groups. The rate of combined events was higher in high-risk patients, although statistically significant only in patients with PVR > 6 WU (OR 1.99, 95% CI 1.17-3.38, p = 0.006). Mortality was also higher in the high-risk groups, with statistical significance for the variables CI (OR 1.8, 95% CI 1.38-3.31, p = 0.038), SVI (OR 3.46, 95% CI 1.51-8.92, p = 0.001), PVR (OR 2.75, 95% CI 1.45-5.34, p < 0.001) and compliance (OR 5.95, 95% CI 2.17-18.86, p < 0.001).
DISCUSSION
The present study represents the analysis of hemodynamic variables with the largest number of patients carried out by a PH working group in our country and confirms the importance of measuring and calculating hemodynamic parameters to determine the patients' prognosis. We decided to include the hemodynamic variables with the best correlation to RV-pulmonary artery coupling and RV work, namely CI and SVI, as SvO2 is a surrogate of CI and RAP is also influenced by the volume overload present in these patients. This study confirms that estimates of CI and SVI are strongly associated with mortality at follow-up. These findings support the concept that RV function and RV-pulmonary artery coupling have a significant impact on patients' survival. However, our analysis questions the need for including other variables in determining prognosis. Beyond the known association of IVS with prognosis, PVR and pulmonary arterial compliance demonstrated an excellent association with the event rate, even greater than the variables suggested by international recommendations. Although the cause of this finding has not been established, a possible hypothesis is that both compliance and PVR continuously worsen from the onset of the disease to the later stages. (12,13) In contrast, cardiac output and stroke volume remain normal due to compensatory mechanisms, only to worsen in advanced stages of PH. (14) In this sense, the absence of association between PAPI and RVSWI and the incidence of events can be explained because both variables not only do not decrease in the initial stages, but also tend to increase during these stages, only to decrease in the final stages of PH. This makes their behavior unpredictable and poorly related to the severity of the disease. (15)
Table 1. Baseline characteristics
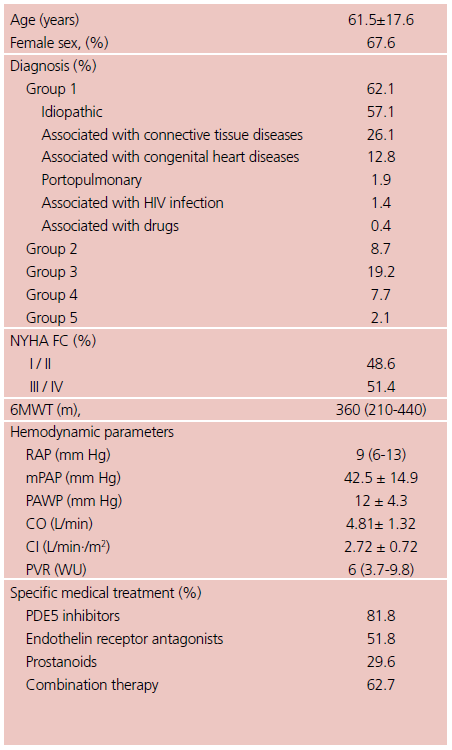
6MWT: 6-minute walking test; CI: cardiac index; CO: cardiac output; HIV: human immunodeficiency virus; mPAP: mean pulmonary arterial pressure; NYHA FC: New York Heart Association functional class; PAWP: pulmonary arterial wedge pressure; PDE5: phosphodiesterase 5; PVR: pulmonary vascular resistance; RAP: right atrial pressure; WU: Wood Units Quantitative variables are presented as mean ±SD or median (IQR) according to their distribution.
These parameters can be very useful in the assessment of the prognosis of PH in entities other than those in group 1. The European guidelines support this assertion by establishing specific medical treatment for PAH in patients with left heart failure or pulmonary parenchymal disease (groups 2 and 3), as long as PVR is > 5 WU. This implies that there is an underlying acknowledgment of the correlation between elevated PVR and the severity of the disease. In addition, in recent years, several clinical trials in PAH have included PVR as a pathophysiologic endpoint to determine the presence or absence of clinical benefit from treatment without considering other hemodynamic variables. (16-18) Both situations, in addition to the findings of not only our study but also others that suggest similar conclusions, underscore the prognostic significance of PVR and compliance as hemodynamic markers. This explains their usefulness both for diagnosis and during follow-up. In fact, an analysis of the REVEAL registry shows that patients with PVR < 5 WU have a 5-year survival rate >70%, while those with higher PVR have a survival rate < 60%. (19)
Table 2. Event rates for each hemodynamic variable
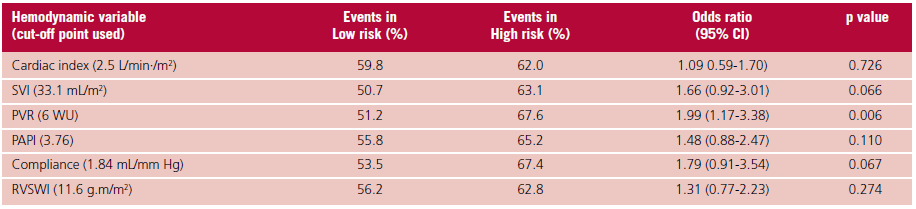
PAPI: pulmonary artery pulsatility index; PVR: pulmonary vascular resistance; RVSWI:right ventricular systolic work index; SVI: stroke volume index.
Table 3. Mortality for each hemodynamic variable
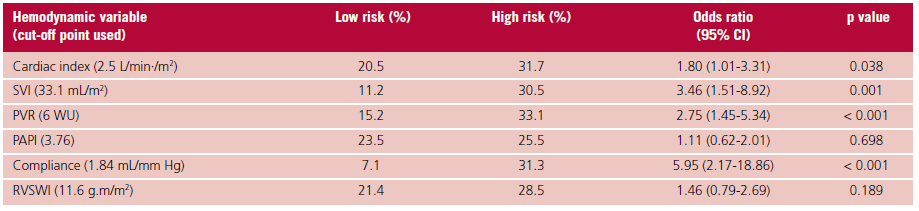
PAPI: pulmonary artery pulsatility index; PVR: pulmonary vascular resistance; RVSWI: right ventricular systolic work index; SVI: stroke volume index.
Our study has some limitations. First, most patients had idiopathic PAH or PAH associated with connective tissue disease, with few patients associated with congenital heart disease, less than in other registries, who usually present with hemodynamic parameters different from the general population with PAH. Second, the hemodynamic variables used as risk parameters are recommended for patients with group 1 pulmonary hypertension, whereas our registry included patients from all groups. This is because most of these risk parameters have been defined based on expert recommendations with little scientific evidence to support them, and are suggested mainly for patients with idiopathic or heritable PAH or associated with drugs. Additionally, they are commonly used for all the groups in clinical practice worldwide, since groups 2 to 5 lack their own risk parameters.
Finally, we did not analyze whether the improvement of worsening of the hemodynamic parameters during follow-up affected the event rate, as indicated by the risk variables recommended by the guidelines. Further follow-up of patients will be required to demonstrate this question.
CONCLUSIONS
Our registry showed that hemodynamic variables used routinely in patients with PH adequately predicted the risk of events. Although RVSWI and PAPI did not have a strong association with events, parameters such as PVR and compliance demonstrated similar or even better risk prediction at follow-up compared to the variables currently used in practice. Additional research is necessary to determine the prognostic significance of different hemodynamic variables for monitoring patients over time.
Conflicts of interest
None declared.
(See conflicts of interest forms on the website).
https://creativecommons.org/licenses/by-nc-sa/4.0/

©Revista Argentina de Cardiología
REFERENCES
- Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J 2022; 43:3618–731. https://doi.org/10.1093/eurheartj/ehac237
- Weatherald J, Boucly A, Chemla D, Savale L, Peng M, Jevnikar M, Jaïs X, et al. Prognostic Value of Follow-Up Hemodynamic Variables After Initial Management in Pulmonary Arterial Hypertension. Circulation. 2018;137:693–704. https://doi.org/10.1161/CIRCULATIONAHA.117.029254
- Thenappan T, Shah SJ, Rich S, Tian L, Archer SL, Gomberg-Maitland M. Survival in pulmonary arterial hypertension: a reappraisal of the NIH risk stratification equation. Eur Respir J 2010;35:1079–87. https://doi.org/10.1183/09031936.00072709
- Nickel N, Golpon H, Greer M, Knudsen L, Olsson K, Westerkamp V, Welte T, Hoeper M. The prognostic impact of follow-up assessments in patients with idiopathic pulmonary arterial hypertension. Eur Respir J 2012;39:589–96. https://doi.org/10.1183/09031936.00092311
- Clapham K, Highland K, Rao Y, Fares W. Reduced RVSWI is associated with increased mortality in connective tissue disease associated pulmonary arterial hypertension. Front Cardiovasc Med 2020;7:77. https://doi.org/10.3389/fcvm.2020.00077
- Ibe T, Wada H, Sakakura K, Ito M, Ugata Y, Yamamoto K, et al. Right ventricular stroke work index as a prognostic indicator for pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension. Int Heart J 2018;59: 1047-51. https://doi.org/10.1536/ihj.17-576
- Baran DA, Grines C, Bailey S, Burkhoff D, Hall S, Henry T, Hollenberg SM, Kapur N, et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock. Catheter Cardiovasc Interv 2019;94:29-37. https://doi.org/10.1002/ccd.28329
- Morine K, Kiernan M, Thinh Pham D, Paruchuri V, Denofrio D, Kapur NK. The Pulmonary Artery Pulsatility Index is Associated with Right REFERENCES Ventricular Failure Following Left Ventricular Assist Device Surgery. J Card Fail 2016;22:110-6. https://doi.org/10.1016/j.cardfail.2015.10.019
- Benza RL, Gomberg-Maitland M, Elliott G, Farber HW, Foreman AJ, Frost AE, et al. Predicting Survival in Patients With Pulmonary Arterial Hypertension. CHEST 2019; 156:323-37. https://doi.org/10.1016/j.chest.2019.02.004
- Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, et al. Survival in Patients With Idiopathic, Familial, and Anorexigen-Associated Pulmonary Arterial Hypertension in the Modern Management Era. Circulation. 2010; 122:156-63. https://doi.org/10.1161/CIRCULATIONAHA.109.911818
- Sitbon O, Benza RL, Badesch D, Barst RJ, Elliott G, Gressin V, Lemarié JC, et al. Validation of two predictive models for survival in pulmonary arterial hypertension. Eur Respir J 2015;46:152-64. https://doi.org/10.1183/09031936.00004414
- Lankhaar JW, Westerhof N, Faes TJ, Gan CT, Marques KM, Boonstra A, et al. Pulmonary vascular resistance and compliance stay inversely related during treatment of pulmonary hypertension. Eur Heart J 2008;29:1688-95. https://doi.org/10.1093/eurheartj/ehn103
- Galié N, RubinL J, Hoeper M, Jansa P, Al-Hiti H, Meyer G, et al. Treatment of patients with mildly symptomatic pulmonary arterial hypertension with bosentan (EARLYstudy): a double-blind, randomized controlled trial. Lancet 2008;371:2093–200. https://doi.org/10.1016/S0140-6736(08)60919-8
- D’Alonzo G E, Barst R J, Ayres S M, Bergofsky EH, Brundage BH, Detre KM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med 1991;115:343–9. https://doi.org/10.7326/0003-4819-115-5-343
- Von Noordegraaf A, Westerhof BE, Westerhof N. The relationship between the right ventricle and its load in pulmonary hypertension. J Am Coll Cardiol 2017;69:236-43. https://doi.org/10.1016/j.jacc.2016.10.047
- Chin K, Sitbon O, Doelberg M, Feldman J, Gibbs S, Grünig E, et al. Three- versus two-drug therapy for patients with newly diagnosed pulmonary arterial hypertension. J Am Coll Cardiol 2021;78:1393-403. https://doi.org/10.1016/j.jacc.2021.07.057
- Jaïs X, Brenot P, Bouvaist H, Jevnikar M, Canuet M, Chabanne C, et al. Balloon pulmonary angioplasty versus riociguat for the treatment of inoperable chronic thromboembolic pulmonary hypertension (RACE). Lancet Respir Med 2022;10:961-71. https://doi.org/10.1016/S2213-2600(22)00214-4
- Hoeper M, Badesch D, Ghofrani HA, Gibbs S, Gomber-Maitland M, McLaughlin V, et al. Phase 3 Trial of sotatercept for treatment of pulmonary arterial hypertension. N Engl J Med 2023;338:1478-90. https://doi.org/10.1056/NEJMoa2213558
- Farber H, Milller D, Poms A, Badesch D, Frost A, Muros-Le Rouzic E, et al. Five-year outcomes of patients enrolled in the REVEAL Registry. Chest 2015;148:1043-54. https://doi.org/10.1378/chest.15-0300