
INTRODUCTION
Cardiac implantable electronic devices (CIEDs), such as implantable cardioverter defibrillators (ICDs) and cardiac resynchronization therapy devices with defibrillator (CRT-D), are a cornerstone in the treatment of patients at risk of sudden cardiac death and those with advanced heart failure. (1) These devices not only deliver life-saving therapies, but also function as sophisticated diagnostic tools that allow continuous collection of large amounts of data on the patient’s heart rhythm and physiological parameters.
Over the last decade, remote monitoring (RM) has transformed the follow-up of this patient population, evolving from a complementary technology to a standard of care recommended by leading international clinical practice guidelines. (2-4) Remote monitoring enables the automatic and scheduled transmission of data from the patient’s device to a monitoring center, facilitating continuous and proactive surveillance, which has consistently shown to reduce the time to detection of actionable clinical and technical events, such as atrial and ventricular arrhythmias or electrode malfunctions.(5-7) In addition, it has proved to be effective in reducing the incidence of inappropriate ICD shocks and decreasing the need for routine in-person visits, thereby optimizing clinical workflows and improving patient convenience. (8-9)
Despite these established benefits, the impact of RM on “hard” clinical outcomes, such as all-cause mortality and hospitalizations, has been an area of intense debate with heterogeneous results in the literature. While some observational studies and clinical trials have suggested an association between RM and improved survival (10-12), other large-scale randomized controlled trials and meta-analyses have reported neutral findings, failing to demonstrate a clear benefit on these primary endpoints. (13-15) This discrepancy highlights the importance of evidence generated in the “real world,” which reflects routine clinical practice in patient populations that are more diverse and complex than those typically included in clinical trials.
Ventricular arrhythmias, ranging from non-sustained ventricular tachycardia (NSVT) to sustained ventricular tachycardia (VT) and ventricular fibrillation (VF), are events frequently detected by RM in patients with ICD/CRT-D. The occurrence of these arrhythmias not only triggers device therapies, but may also be a marker of progression of the underlying heart disease and an indicator of poor prognosis. (16) Therefore, understanding the incidence of these alerts and their association with long-term outcomes such as survival is of utmost clinical importance.
The aim of this study was twofold: first, to characterize demographically and clinically our cohort of patients with ICD and CRT-D followed-up with RM in a routine practice setting in Argentina; and second, to evaluate the prognostic value of ventricular arrhythmia alerts (VT, VF, or NSVT) on all-cause survival in this population.
METHODS
A descriptive, retrospective cohort study was conducted in a closed-population hospital of the Autonomous City of Buenos Aires. A database was built from the records of patients with CIEDs. For the present analysis, all patients with an ICD or CRT-D implanted between August 2018 and January 2025 and with an active RM system were selected. The exclusion criteria were: 1) patients with devices other than ICDs or CRT-Ds, 2) documented follow-up of less than 6 months, and 3) incomplete data on key variables such as the date of implantation or vital status at the end of follow-up. The final cohort who met all the criteria for analysis consisted of 62 patients.
Data were obtained from two main sources, linked through a unique patient identifier: a patient management database and a systematic record of alerts received through RM platforms.
The following baseline variables were collected: age at the time of implantation, gender, device type (ICD vs. CRT-D), history of atrial fibrillation prior to implantation, use of baseline anticoagulation, and comorbidities such as hypertension, diabetes mellitus, diagnosis of heart failure, and chronic kidney disease. Drugs such as sodium-glucose cotransporter 2 inhibitors were not analyzed, since a significant number of patients began follow-up in the cohort prior to the publication of the studies that established their use as standard of care. Dual angiotensin-nepril ysin inhibitors were also not included in the baseline analysis, as these data were not systematically collected in the retrospective database.
The date of device implantation, the date of the last check-up or death, and vital status were recorded during follow-up. Based on these dates, the follow-up time and survival time in days were calculated for each patient.
All alerts transmitted and classified by the device as NSVT, VT, or VF were analyzed. Each alert documented whether the event was symptomatic and whether it generated an unscheduled visit. The device response to the alert was categorized as “Monitor”, “ATP” (anti-tachycardia pacing therapy), or “Shock.” Subsequent clinical management was categorized as “Pharmacological Adjustment”, “Inappropriate Shock Programming Adjustment”, or other. A dichotomous variable was created to classify patients into two groups: those who had at least one of these alerts during follow-up and those who did not.
The standard baseline programming used for alerts followed the recommendations of international guidelines for reducing inappropriate therapies. (17) A VT monitoring zone was established, with a detection threshold of 340 ms (> 176 bpm) and a counter of 28 intervals for detection. In this zone, sudden onset (Onset 20%), Stability (48 ms), and morphology discriminators were programmed as active. The therapy zone (VF) was programmed with an interval of 320 ms (> 188 bpm) and a counter of 18 out of 24 intervals for detection, with ATP (Burst) therapies followed by shocks.
It should be noted that this was the baseline programming; in secondary prevention patients or after an episode, this programming could be individualized. However, these values were used as the minimum criteria for defining events.
With this programming, the 40 alerts analyzed were classified as: NSVT alerts (n=4), defined as non-sustained episodes (e.g., duration less than 28 beats) that only generated a “Monitor” alert; and VT/VF alerts (n=36), defined as sustained episodes that reached the detection counter in the therapy zone and received ATP or shock.
All 40 alerts analyzed were manually confirmed by a staff electrophysiologist to validate their ventricular origin and exclude artifacts or supraventricular tachycardias.
Statistical analysis
Descriptive statistics were used to summarize the cohort characteristics. Continuous variables were presented as mean±standard deviation (SD) or median and interquartile range and categorical variables were expressed as absolute frequencies (n) and percentages (%).
Baseline characteristics between the group of patients with alerts and those without alerts, were compared with Fisher’s exact test for all categorical variables, and for the continuous variable “Age at Implantation,” with a non- normal distribution, the Mann-Whitney U test was used.
For survival analysis, the event of interest was defined as all-cause mortality. The time to event was calculated from the device implantation date to the date of death or the date of the last follow-up. The Kaplan-Meier method was used to estimate and visualize survival probabilities over time for each group. The Log-Rank test was used to formally compare the survival curves.
A value of p < 0.05 was considered statistically significant. All analyses were performed using R version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria).
Ethical considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki. (18) Data confidentiality was ensured by anonymizing the final database. All patients had given an informed consent at the start of remote monitoring, authorizing the use of their data for research purposes. Given the retrospective and anonymized nature of the analysis, the need for specific approval by the institutional ethics committee was waived from the study.
RESULTS
Baseline Cohort Characteristics
A total of 62 patients with ICD or CRT-D were included in the analysis. The baseline demographic and clinical characteristics of the cohort are summarized in Table 1. Mean age at implantation was 61.8 years (median 64; range 16-87). The population was predominantly male (47 patients, 75.8%). The mean follow-up time was 2.61 years (median 2.2 years; range 0.6-7.2).
Table 1
Baseline characteristics of the cohort of patients with ICD/CRT-D (N= 62 )
| Characteristic | Variable |
|---|---|
| Age at Implantation (years) | |
| - Median (IQR) | 64.8 (55.8-73.8) |
| - Range (Min-Max) | 16-87 |
| Gender, n (%) | |
| - Male | 47 (75.8%) |
| - Female | 15 (24.2%) |
| Type of device, n (%) | |
| - ICD only | 49 (79.0%) |
| - CRT-D | 13 (21.0%) |
| Baseline Comorbidities, n (%) | |
| - AF Prior to Implantation | 7 (11.3%) |
| - Baseline Anticoagulation | 13 (21.0%) |
| - Heart Failure | 41 (66.1%) |
| - Hypertension | 53 (85.5%) |
| - Diabetes Mellitus | 19 (30.6%) |
| - Chronic Kidney Disease | 16 (25.8%) |
| LVEF (median, IQR) | 30.0% (22-34) |
| Etiology, n (%) | |
| - Ischemic | 19 (30.6%) |
| - Non-ischemic | 42 (67.7%) |
| Functional class (NYHA), n (%) | |
| - NYHA I | 45 (72.6%) |
| - NYHA II-IV | 17 (27.4%) |
| Baseline Medication, n (%) | |
| - Beta-blockers | 55 (88.7%) |
| - RAAS blockade | 49 (79.0%) |
| - MRA | 39 (62.9%) |
| - Amiodarone | 31 (50.0%) |
| Follow-up time (years) | |
| - Median (IQR) | 2.2 (1.2 - 3.6) |
| - Range (Min-Max) | 0.6-7.2 |
AF: Atrial fibrillation; CRT-D: Cardiac resynchronization therapy with defibrillator; ICD: Implantable cardioverter defibrillator; IQR: interquartile range; LVEF: Left ventricular ejection fraction; MRA: Mineralocorticoid receptor antagonist; NYHA: New York Heart Association; RAAS: Renin-angiotensin-aldosterone system
Incidence and Management of Ventricular Arrhythmia Alerts
During the follow-up period, 22 of the 62 patients (35.5%) presented a total of 40 alerts for ventricular arrhythmias (VT, VF, or NSVT). Of these 40 alerts, 15 (37.5%) were symptomatic and 17 (42.5%) led to an unscheduled consultation.
The device response associated with these alerts was: only monitoring in 4 cases (10%), anti-tachycardia pacing (ATP) therapy in 11 (27.5%), and shock therapy in 25 (62.5%). The documented clinical management following the alerts consisted of no change in 24 cases (60%), pharmacological adjustment in 11 (27.5%), programming adjustment in 4 (10%), and referral for ablation in 1 (2.5%). It should be noted that, of the 25 shocks, 3 (12%) were followed by reprogramming because they were considered inappropriate. Details of management according to device response are summarized in Table 2.
Table 2
Clinical management according to device response to ventricular arrhythmia alerts (N=40 alerts)
| Device Response | Pharmacological Adjustment | Programming Adjustment | Ablation | No Change | Total Alerts |
|---|---|---|---|---|---|
| Monitor | 0 | 0 | 0 | 4 | 4 |
| ATP | 2 | 1 | 0 | 8 | 11 |
| Shock | 9 | 3* | 1 | 12 | 25 |
| Total | 11 | 4 | 1 | 24 | 40 |
ATP: anti-tachycardia pacing
*Corresponds to “Inappropriate Shock Programming Adjustment”
Comparative Subgroup Analysis
The baseline characteristics of patients who presented ventricular arrhythmia alerts (n=22) were compared with those who did not (n=40), as detailed in Table 3. There was a trend toward older age (median 67 vs. 62 years; p=0.063) and a higher prevalence of hypertension (95.5% vs. 77.5%; p=0.082) in the group with alerts. Left ventricular ejection fraction (LVEF) was significantly lower in the subgroup with alerts, and the prevalence of major heart failure (Table 3) The most relevant finding was the statistically significant association between the occurrence of ventricular alerts and higher all-cause mortality (40.9% vs. 7.5%; p=0.003), with an odds ratio of 8.54 (95% CI 2.0541.5, p=0.003).
Table 3
Comparison of baseline characteristics between patients with and without ventricular arrhythmia alerts
| Baseline Characteristic | Patients with alerts (N=22) | Patients without alerts (N=40) | Ratio (95% CI) | p-value |
|---|---|---|---|---|
| Age at Implantation (years, median) | 67 | 62 | - | 0.063 |
| Male gender | 86.4 % | 70.0 % | 0.218 | |
| CRT-D | 31.8 % | 15.0 % | 0.191 | |
| AF prior to implantation | 13.6 % | 10.0 % | 0.691 | |
| Heart failure | 77.3 % | 60.0 % | 0.262 | |
| Hypertension | 95.5 % | 77.5 % | 0.082 | |
| Diabetes Mellitus | 22.7 % | 35.0 % | 0.395 | |
| Chronic kidney disease ( ) | 31.8 % | 22.5 % | 0.546 | |
| LVEF (median) | 28.5 % | 38% | - | 0.003 |
| Ischemic etiology | 45.5 % | 22.5 % | 0.085 | |
| NYHA II-IV | 54.5 % | 12.5 % | 0.005 | |
| Beta blockers | 95.5 % | 85.0 % | 0.371 | |
| RAAS blockade | 100 % | 67.5 % | 0.002 | |
| MRA | 86.4 % | 50.0 % | 0.005 | |
| Amiodarone | 50.0 % | 50.0 % | 1.000 |
AF: atrial fibrillation; CRT-D: cardiac resynchronization therapy with defibrillator; LVEF: left ventricular ejection fraction; MRA: mineralocorticoid receptor antagonists; NYHA: New York Heart Association; RAAS: renin-angiotensin-aldosterone system
Survival Analysis
To assess the prognostic impact of ventricular arrhythmia alerts on all-cause mortality, a survival analysis was performed using the Kaplan-Meier method. Survival over time was compared between the group of patients who had at least one VT, VF, or NSVT alert (n=22) and the group who did not have such alerts (n=40).
Figure 1 shows the survival curves for both groups. A clear and early separation of the curves was observed, with a consistently lower probability of survival over time in the group of patients with alerts compared with the group without alerts.
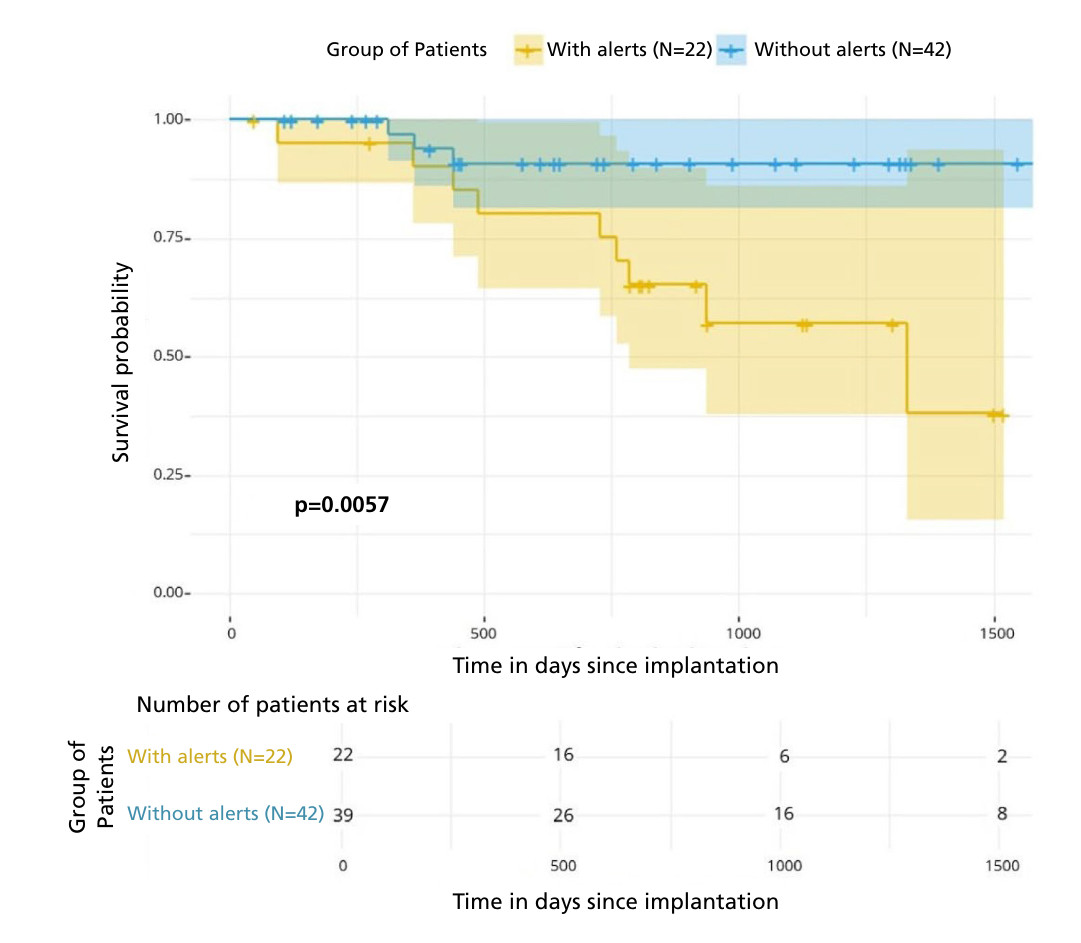
The Log-Rank test confirmed that this difference in survival was highly statistically significant (p= 0.006). To adjust for heterogeneous follow-up duration (range 0.6-7.2 years), annualized mortality was calculated by group. This was markedly higher in the alert group (18.33 deaths per 100 person-years) compared with the no-alert group (2.74 deaths per 100 person-years).
These findings indicate that the occurrence of ventricular arrhythmia alerts, detected by remote monitoring, was a strong predictor of increased mortality in our cohort of patients with ICD/CRT-D.
DISCUSSION
This real-world study characterizes a cohort of patients with ICD/CRT-D and demonstrates that the occurrence of ventricular arrhythmia alerts detected by RM is a powerful marker of poor prognosis. The main finding of our study is the statistically significant association between the presence of VT, VF, or NSVT alerts and an increase in all-cause mortality. The Kaplan-Meier survival analysis not only confirms this finding but also allows us to visualize how risk diverges over time, with a notable separation of the curves after 500 days.
This result aligns our experience with that of other studies that have identified ventricular arrhythmias as an independent risk factor for mortality in this population. (16,19) The ability of RM for the early detection of these events is therefore crucial not only for the immediate management of the arrhythmia but also for long-term risk stratification. It is important to contextualize our findings with those of large international studies, although with differences in their objectives. Unlike randomized trials such as REM-HF (9) or studies as REMOTE-CIED, (14) which reported neutral findings on the impact of RM on all-cause mortality, our study does not evaluate RM per se, but rather the prognostic value of the alerts detected. In this sense, our results are in line with those of large observational registries, such as the ALTITUDE study (11), which did suggest an association between RM and improved survival. (20) The nearly sevenfold difference in the exposure-adjusted mortality rate reinforces the Kaplan-Meier curve finding and suggests that the association between ventricular alerts and worse prognosis is robust, rather than a mere artifact of differential follow-up. (21)
The ability of RM for the early identification of high-risk patients, such as those with ventricular arrhythmias, remains of fundamental clinical value. A patient presenting with these alerts may be a candidate for intensification of heart failure therapy, reevaluation of antiarrhythmic therapy, or consideration of more advanced therapies such as ablation.
We are aware of the limitations of our study. Its retrospective and observational design does not allow us to establish causality but only association, and the modest cohort size (n=62) limits statistical power.
The main limitation is the absence of multivariate analysis (e.g., Cox regression) to adjust for obvious confounding factors. As shown in the comparative analysis (Table 3), the group that presented alerts had a significantly higher baseline risk profile: a markedly lower median left ventricular ejection fraction (LVEF), a greater prevalence of ischemic etiology, a much higher proportion of symptomatic patients according to the New York Heart Association (NYHA IIIV) functional classification and a greater use of heart failure medication (such as mineralocorticoid receptor antagonists and renin-angiotensin-aldosterone system blockade).
Although a Cox analysis was considered, because of the low number of mortality events in the cohort (n=12), attempting to adjust for multiple confounders would result in overfitting of the model, generating statistically unstable and unreliable results. Therefore, the reported odds ratio for mortality probably overestimates the actual association, as it is an unadjusted calculation.
CONCLUSION
In conclusion, in our cohort, the occurrence of remote monitoring alerts for ventricular arrhythmias was a frequent finding and was significantly associated as a prognostic marker of lower survival. This finding underscores the prognostic value of information obtained through RM and its importance for risk stratification and clinical decision-making in patients with implantable defibrillators.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web).