INTRODUCTION
In apparently healthy individuals,
the risk of a future cardiovascular
event is related to the number and intensity
of risk factors
and the duration
of exposure. (1)
The best known strategy in
cardiovascular prevention is to use risk scores to identify those individuals at high risk of developing cardiovascular
disease and to recommend preventive
measures according to the calculated risk level. (1,2) Risk scores
or risk functions are
mathematical equations that calculate the probability that an individual will
develop the event of interest within a specific period of time, according to
the level of exposure to different risk factors. (3) However, these
scores have major limitations related to calibration, discrimination and low
sensitivity, as most cardiovascular events occur in the population group with low or intermediate risk. (4)
Several additional biomarkers have
been evaluated to improve cardiovascular risk stratification (risk modulators). (5) Detection of carotid atherosclerotic plaques
(CAP) improves the prediction of cardiovascular events over and above that
provided by models that only consider
conventional risk factors. (6,7) Coronary artery
calcium (CAC) score is associated strongly and in a graded
fashion with the risk of presenting
cardiovascular events, independently of age, sex, ethnicity, and traditional risk factors. (8,9) Finally, elevated lipoprotein(a) [Lp(a)]
levels are independently associated
with increased cardiovascular risk due to the
activation of atherogenic, inflammatory and prothrombotic mechanisms. (10)
Considering the above, the aims of this study were:
1) to determine the prevalence of risk modulators [CAP, CAC score
and Lp(a) level] in a primary pre vention population initially stratified through a risk score; 2) determine the concordance
between the 2 methods of detecting
subclinical atheromatosis (CAP and CAC score); 3) establish which proportion of patients should
receive statins according to the initial risk stratification and after being recategorized by screening
for risk modulators.
METHODS
This is a descriptive
cross-sectional study with a sample obtained
from the cardiovascular prevention outpatient clinic belonging to the Department of
Cardiology of a private health center in the Autonomous City of Buenos Aires.
Patients between 18 and 79 years,
without cardiovascular disease or previous lipid-lowering treatment who attended
the clinic for cardiovascular risk assessment were included.
Definition of variables
The risk score (ASCVD Risk
Estimator) used by the American guidelines for the management of cholesterol
(American College of Cardiology/American
Heart Association) was calculated in patients within the age range and with the
variables required to calculate it. (11) Patients with a score
< than 5%, between 5% and 7.4%, between 7.5% and 19.9%, and equal to or greater than 20% were classified
as low risk, "borderline" risk, moderate
risk, and high risk, respectively. The presence of CAP was non-invasively assessed
by ultrasound and was defined as: 1) abnormal wall thickness (defined
as intima-media thickness
> 1.5 mm); 2) abnormal structure (protrusion towards the lumen, loss of alignment
with the adjacent wall); and 3) abnormal wall echogenicity. The CAC score was calculated using a multislice computed
tomography without contrast
agent injection and with
electrocardiographic gating during a breath-hold of approximately 5-7 seconds.
Coronary calcium was identified as an
area of at least 1 mm2 at the level of the vessel with a threshold > 130 Hounsfied units. The CAC
score obtained was expressed
in Agatston units.
Lp(a) plasma level was obtained by the nephelometric method and was expressed in mg/dL. A value of 50 mg/dL or greater
was considered elevated. Triglyceride levels, total cholesterol and HDL-cholesterol (HDL-C) were measured by enzymatic-colorimetric assay method and
immunoturbidimetry.
LDL-cholesterol (LDL-C) was calculated with the Friedewald
formula. (12) Glomerular filtration rate was estimated using the CKD-Epidemiology Collaboration (CKD- EPI) equation. (13) All the tests were performed in a single laboratory with the same methods.
For this study, and based on
current recommendations, statins were indicated for the following
groups of patients
in primary prevention, after the initial
stratification by clinical data and risk score: a) severe
hypercholesterolemia (C-LDL 190 mg/dL); b) diabetes mellitus; c) moderate or severe renal dysfunction (glomerular filtration rate < 60 mL/min/1.73 m2); d) high risk score.
(11-15) With the information obtained about the presence
of risk modulators, the following
clinical scenarios were also considered for recommending statins according to
different guidelines, position papers,
and consensus statements: (a) patients with borderline or moderate risk with
CAC score > 0 (14); (b) low-risk patients with a
CAC score 100 or greater than the expected
75th percentile for sex and age (11,15,16); c) patients with low, borderline or moderate risk with CAP (12,13); d) subjects with moderate risk and a Lp(a)
value 50 mg/dL (17);
and e) subjects with low or borderline
risk and a Lp(a) value 75 mg/dL. (17)
Statistical analysis
The normal distribution of the variables was explored by analyzing mean, standard deviation, median, skewness, kurtosis, a histogram and with the Shapiro-Wilk test. The difference of continuous
variables between the groups were compared using the Student's t test or Mann-Withney-Wilcoxon test for normal and abnormal distributions, respectively. Categorical variables were analyzed
with the chi-square test. The
agreement between the two methods for quantifying subclinical atheromatosis (CAC by computed tomography and CAP by ultrasound) was analyzed using
Fleiss' kappa. Agreement was defined as poor, fair, moderate, substantial, or almost perfect if the kappa value was less than or equal to 0.20, between
0.21 and 0.40, between 0.41 and 0.60, between
0.61 and 0.80, and between 0.81 and 1, respectively. Continuous variables were expressed as mean ± standard
deviation or median (25-75 interquartile range), as applicable, and categorical variables
as percentages. A twotailed p value < 0.05 was considered statistically significant. All the statistical calculations were performed
using STATA 11.1 software
package.
Ethical considerations
The study was conducted
following the recommendations regarding medical
research of the Declaration of Helsinki, the Guidelines for Good Clinical
Practice and the current ethical rules.
RESULTS
A
total of 348 patients in primary prevention who were not receiving
lipid-lowering treatment were included in our study. Mean age was 55.6 ± 12.2 years and 45.4%% were men; 8.1% had a history of
type 2 diabetes mellitus and 40.2%
had hypertension. Mean total
cholesterol was 242.5 ± 51.9 mg/dL. The characteristics
of the study population are described in Table 1.
Table 1. Characteristics of the population
included in the study
|
Continuous variables, mean ± SD or median (IQR) |
n = 348 |
|
Age, years |
55.6 ± 12.2 |
|
Systolic
blood pressure, mm Hg |
130.4 ± 16.5 |
|
Body mass index, kg/m2 |
27.4
± 5.0 |
|
Total
cholesterol, mg/dL |
242.5 ± 51.8 |
|
HDL-C, mg/dL |
52.5
± 15.7 |
|
LDL-C,
mg/dL |
156.7 ± 48.1 |
|
Triglycerides, mg/dL |
140.5
(88-201.5) |
|
Apolipoprotein
B, mg/dL |
126.3 ± 34.3 |
|
Creatinine, mg/dL |
0.9
± 0.5 |
|
Risk
score*, % |
7.3 (3.2-15.2) |
|
Categorical variables, n (%) |
|
|
Male
sex |
158 (45.4) |
|
Current smoker |
49
(14.1) |
|
Type
2 diabetes mellitus |
28 (8.1) |
|
Hypertension |
140
(40.2) |
|
Obesity |
76 (22.4) |
|
FH |
126
(36.3) |
|
Risk
strata* Low risk "Borderline" risk Intermediate risk High risk |
109 (37.9) 41 (14.2) 94 (32.6) 44 (15.3) |
FH: family history
or early cardiovascular disease; HDL-C: HDL-cholesterol; LDL-C:
LDL-cholesterol; SD: standard deviation; IQR: 25-75 interquartile risk.
*The risk score used was the ASCVD Risk Estimator (American College of Cardiology/American Heart Association)
and was calculated in 288 patients.
The adequate characteristics to
estimate the risk score were found in
82.8% (n = 288) of the population.
When this subpopulation was analyzed, 37.9%,
14.2%, 32.6% and 15.3% of patients were classified at low, "borderline", moderate
or high risk,
respectively.
The risk score could not be
estimated in 17.2% (n = 60) of the population
due to age < 40 years (n = 37), presence of severe hypercholesterolemia, total cholesterol > 320 mg/dL, (n = 20) or both conditions (n = 3).
Overall, 29.8%, 36.8%, and 53.2% of patients showed a Lp(a) value 50 mg/dL, CAP, or a CAC score 0, respectively. A CAC score 100
or 300 was present in 17.5%
and 8.3% of subjects, respectively, while only 5 patients had a score 1000.
Patients with elevated Lp(a)
levels showed higher total
cholesterol, LDL-C, HDL-C and apolipoprotein B values compared with those with low
levels. Patients with CAP were older and were more commonly
hypertensive compared to patients without carotid atheromatosis.
Finally, risk factors (including age, male sex, lipid values, obesity, diabetes, and hypertension) were more common in individuals with a CAC score > 0 compared with patients with a CAC score = 0. The characteristics of the population according to the presence or absence
of risk modulators are shown in Table 2.
![]()
![]()
![]()
![]()
![]()
![]() Table 2. Characteristics of the population
according to the presence or absence of risk modulators
Table 2. Characteristics of the population
according to the presence or absence of risk modulators
|
Continuous variables, mean ± SD or median (IQR) |
Lp(a)
< 50 mg/dL (n = 244) |
|
Without atherosclerotic plaque (n = 220) |
With atherosclerotic plaque (n = 128) |
CAC score = 0 (n = 163) |
CAC score > 0 (n = 185) |
|
Age,
years |
54.3 ± 13.2 |
56.5 ± 12.6 |
52.6 ± 12.2 |
62.4 ± 11.1* |
51.2 ± 12.9 |
60.6 ± 11.1* |
|
Systolic blood pressure, mm Hg |
127.6 ± 16.8 |
130.5 ± 17.6 |
127.4 ± 15.6 |
136.1 ± 16.9* |
126.1 ± 15.9 |
134.6 ± 16.2* |
|
Body
mass index, kg/m2 |
26.9
± 4.9 |
26.7
± 4.0 |
27.1
± 5.3 |
27.6
± 4.6 |
26.1
± 4.3 |
28.3
± 5.4* |
|
Total cholesterol, mg/dL |
242 ± 53.4 |
271.2 ± 57.6* |
238.4 ± 47.9 |
247.2 ± 57 |
233.8 ± 40.6 |
248.4 ± 58.7* |
|
HDL-C,
mg/dL |
52
± 15.6 |
56.9
± 16.1* |
52.6
± 16 |
53
± 15.3 |
55.1
± 16.9 |
50.1
± 14.4* |
|
LDL-C, mg/dL |
156.4 ± 47.9 |
178.6 ± 59.4* |
152.9 ± 43.6 |
160.9 ± 54 |
149.2 ± 35.9 |
161.6 ± 55.5* |
|
Triglycerides,
mg/dL |
132.5 (83.5-194.5) |
141.5 (88-197) |
135.5 (87-207) |
145 (89-195) |
121.5 (84.5-185.5) |
152 (93-218)* |
|
Apolipoprotein B, mg/dL |
123.7 ± 35.3 |
137.5 ± 33.1* |
123.8 ± 32.2 |
128.7 ± 37.4 |
119.7 ± 27.9 |
131.2 ± 38.7* |
|
Creatinine levels,
mg/dL |
0.92
± 0.6 |
0.84
± 0.2 |
0.84
± 0.2 |
0.95
± 0.7 |
0.85
± 0.2 |
0.91
± 0.6 |
|
Categorical variables, % |
||||||
|
Male
sex |
47.1 |
34.4 |
44.1 |
45.9 |
37.8 |
50.8* |
|
Current smoker |
13.1 |
14.1 |
12.6 |
15.6 |
12.2 |
15.1 |
|
Type
2 diabetes mellitus |
7.2 |
7.8 |
8.1 |
7.4 |
4.3 |
10.9* |
|
Hypertension |
34.0 |
35.9 |
32.9 |
55.6* |
26.8 |
53.9* |
|
Obesity |
22.7 |
17.5 |
23.4 |
20.9 |
15.8 |
27.9* |
|
FH |
35.3 |
42.2 |
32.5 |
38.3 |
36.7 |
34.1 |
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]() FH: family history or early cardiovascular disease; HDL-C: HDL-cholesterol; LDL-C: LDL-cholesterol; SD: standard deviation; Lp(a): lipoprotein(a); CAC: coronary artery calcium; IQR: 25-75 interquartile risk.
FH: family history or early cardiovascular disease; HDL-C: HDL-cholesterol; LDL-C: LDL-cholesterol; SD: standard deviation; Lp(a): lipoprotein(a); CAC: coronary artery calcium; IQR: 25-75 interquartile risk.
*p < 0.05
In the subpopulation stratified by
risk score (n = 288), 27.2% had Lp(a) levels
50 mg/dL, with a median
of 25 (9.9-57.7) mg/dL. Coronary calcium
score was 0 in 55.9% of the subjects
and 39.2% presented CAP. In addition,
CAC score was 100 or the 75th percentile expected for sex and age in 18.9% and 29.6% of patients.
The presence of risk modulators in the different categories estimated by the
cardiovascular risk score can be
observed in Figure 1. Despite the lack of indication
for statins, a significant proportion of low-
risk subjects (n = 109) had risk modulators: 25.7% had Lp(a) 50 mg/dL; 22% had CAP; 33% had
CAC score > 0, and 33% had CAC score 75th percentile for sex and age.

Fig. 1. Prevalence of risk mod ulators in the different categories of cardiovascular risk factors
(n = 288) *p < 0.05.
Lp(a): Lipoprotein(a); p75: percentil 75; CAC: coronary artery
calcium.
In the subpopulation that could
not be stratified using the risk score due to age < 40 years and in those with total cholesterol < 320 mg/dL (n = 37), median Lp(a) was 18.6
(9.8-36.3) mg/dL, and was 50 mg/dL in 18.9% of patients. In 8.1% of patients CAC score was > 0 and 2.7% had CAP, with an overall
prevalence of subclinical atherosclerosis of 11%. It is worth mentioning that in subjects < 45 years
and with total cholesterol < 320 mg/dL (n = 60) the prevalence of CAP was 18.3% while
10% had CAC score > 0 (none of the patients
had CAC score 100). The total prevalence of
subclinical atheromatosis
in subjects < 45 years was 23%. Figure 2 shows the graphical
representation of the prevalence of cardiovascular
risk modulators in this subpopulation.

Fig. 2. Prevalence of risk modulators in the patients
< 40 years (n = 60).
Lp(a): Lipoprotein(a); p75: percentil 75; CAC: coronary artery
calcium.
In the subpopulation that could
not be stratified using the risk score due to severe hypercholesterolemia (n = 23), the median Lp(a) was
54.3 (20-72) mg/dL and was 50 mg/dL in 55% of
patients. In addition, 91.3% and 65.2% of
patients had a CAC score > 0 or
associated CAP, respectively. In
addition, 25% and 66.7% of patients
had CAC score 100 or 75th percentile expected for age. The graphical
representation of the prevalence of
cardiovascular risk modulators in this subpopulation can be observed
in Figure 3.

Fig. 3. Prevalence of risk modulators in the patients
with severe hypercholesterolemia (>320 mg/dL, n = 23). Lp(a): Lipoprotein(a); p75: percentil 75; CAC: coronary artery
calcium.
Of the total of patients with CAP,
75.8% had a CAC score > 0. Moreover, of all the patients with a CAC score > 0,
52.4% had CAP. The agreement between the two
methods for quantifying subclinical atheromatosis was fair (kappa= 0.33), both in men (kappa = 0.35)
and women (kappa = 0.30). In patients 40 years, agreement was fair (kappa = 0.29),
and was moderate (kappa = 0.45) in younger
patients.
The initial stratification based on
clinical data and risk score showed that 33% (n = 115) of the population would be candidates to receive statins. However, when the presence of risk modulators was
considered, 110
patients (47.2%) who were initially not considered candidates for lipid-lowering
agents had indication for statins (Figure 4).
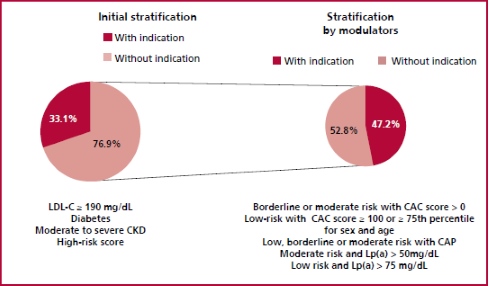
Fig. 4. Indication of statins by baseline stratification and after screening for risk modulators CAC: coronary artery calcium; CKD: chronic kidney
dysfunction; Lp(a): Lipoprotein(a); CAP: carotid artery plaque.
DISCUSSION
Our study exposes the limitations
of estimating cardiovascular risk based exclusively on a risk score, since many young patients or with low-risk
score had subclinical atheromatosis or elevated lipoprotein(a) levels.
In our study, the risk score
could not be assessed in 37
subjects < 40 years without severe hypercholesterolemia. In the 60 patients
< 45 years despite
the CAC score was available,
we could not evaluate the percentile >75th by sex and age, since the epidemiological
studies did not report the percentiles in this age group. These results are clinically relevant since approximately
3% to 10% of acute coronary syndromes occur
in very young patients. (18) Despite these results,
cardiovascular risk is often underestimated in
this population. Very young patients with a first episode of coronary
artery disease have high prevalence of
overweight, smoking and hyperlipidemia. (19) Our data showed that approximately 1 out of 4 to 5 subjects < 45 years had subclinical atheromatosis
(18% CAP, 10% CAC score > 0). Similar findings
were recently reported in a study by Razavi et al. in
which 1 out of 10 young people in the
general population and one out of
three young people with traditional risk factors
had a high CAC score. (20) In addition, a cohort
study including more than 13 000 subjects aged
30-49 years reported
a prevalence of CAC score
> 0 in 20.6%. At
long-term follow-up, CAC score was an independent
predictor of vascular events and mortality. (21) Also, another study evaluated the presence of subclinical atheromatosis in a very
young population (between 14 and 40
years old). The prevalence of CAP was
5.2%, and even more relevant, its presence was
independently associated with a higher incidence of cardiovascular events and mortality during
follow-up. (22)
On the other hand, although our
study showed that the higher risk estimated with the
risk score was associated with higher
prevalence of subclinical atheromatosis, one third of
the patients categorized as "low risk"
had CAC score > 0 and 1 out of 5
subjects had CAP. Similar
results were reported
in previous studies,
in which 20-30% of patients categorized as "low risk" by different scores
exhibited CAP. (23, 24) Likewise, in large population-based studies,
11% to 15% "low-risk" patients were recategorized
when CAC score was considered. (25) Although the
percentages are lower than those
reported in our paper, our sample of patients is made up of individuals who consulted for cardiovascular risk
assessment and had a higher prevalence of risk factors compared to the general population.
Subjects with severe
hypercholesterolemia (many of them with familial
hypercholesterolemia), who could not be stratified using the risk
score constitute a population at
increased cardiovascular risk. Although the presence
of risk modulators in this population adds prognostic information, (26-29) it does not change the initial indication for high-intensity
statins. Our study showed a high
prevalence of risk modulators in this subpopulation,
in agreement with other publications. Only less than 9% of patients
with severe hypercholesterolemia had no subclinical
coronary atheromatosis, whereas 65% had atherosclerotic involvement of both territories.
The current evidence suggests that
estimation of CAC score better predicts
cardiovascular events than the
presence of CAP. (30) However, the
agreement between both determinations to detect subclinical atheromatosis
was low in our study. In other words, and consistent
with the data we have previously reported, a
"normal" carotid Doppler ultrasound does not exclude the presence of subclinical
coronary artery atherosclerosis, and vice versa. (31) Furthermore, our findings
coincide with those reported by Moreyra et al. in that the agreement between the
coronary and carotid territories in subjects undergoing primary prevention was weak (kappa 0.21). (32)
Another interesting finding of our paper is that approximately 25-30%
of patients showed
an elevated Lp(a) level, including
the low-risk subgroup.
Except for lipid profile,
there was no significant association between
high Lp(a)
values and traditional risk factors. The association between elevated Lp(a) values and increased
risk of cardiovascular disease has emerged from
epidemiological and genetic studies. (33,34) The activation of pro-atherogenic, pro-inflammatory and pro-thrombotic mechanisms would explain the association of this
lipoprotein with increased cardiovascular risk.
(35) Recently, a European position paper recommends measuring
Lp(a) concentration at least once in a lifetime in the adult population.
Without specific therapies to reduce Lp(a)
levels, this consensus recommends counteracting elevated Lp(a)
by early and intensive control
of risk factors, mainly by treating hypertension and reducing LDL-C. (17)
In addition, several guidelines on cardiovascular prevention recommend screening for
subclinical atheromatosis, mainly in "intermediate risk" patients, as a
useful means of recategorizing them. (11,14, 16) The main aim
of recategorization is to better identify patients
who will benefit from the use of statins. Lipid guidelines, recommendations, and consensus statements also use the detection of risk
modulators to rec ommend C-LDL targets and the intensity of lipid-lowering therapy.
(11-16) Our work showed that 47.2% of the subjects who were not initially
candidates for receiving statins,
were so when they were reclassified through
the detection of risk modulators. Therefore, using this hybrid modality
of vascular risk assessment,
we would recommend the indication of statins
in 65% of our population sample. In our opinion, and considering our results, screening for
risk modulators should also be considered in low-risk strata.
Finally, the strategy of
estimating cardiovascular risk based
on risk scores was practically not evaluated
in randomized clinical trials. Recently, a study showed that risk stratification based on CAC
score compared with a strategy based
on risk score may be more efficient, personalized, cost-effective, and motivating for statin initiation and maintenance in patients in primary
prevention. (36) Whether this further translates into a reduction in
cardiovascular events is being evaluated in a large, long-term trial. (37)
Our study has certain
limitations. Firstly, in we only
used the risk score recommended by the American guidelines. The implementation of other risk functions could change the results. Secondly,
the criteria used to indicate
statins were selected by the group of
researchers, based on current local and international guidelines. Finally, the
presence of biases and confounders may be expected
due to the observational design
of our study.
CONCLUSION
The presence of risk modulators
was common in this population in primary prevention, even in low-risk
subjects or young individuals. Considering simultaneous screening of several
risk modulators could optimize the initial stratification of our patients and
lead to reconsider treatment with statins.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web/Additional material.)
![]() https://creativecommons.org/licenses/by-nc-sa/4.0/
https://creativecommons.org/licenses/by-nc-sa/4.0/
©Revista Argentina
de Cardiología
1. Graham IM, Di Angelantonio E, Visseren F, De Bacquer D, Ference BA, Timmis A, et al. Systematic
Coronary Risk Evaluation (SCORE): JACC Focus Seminar 4/8. J Am Coll
Cardiol 2021;77:3046- 57. https://doi.org/10.1016/j.jacc.2021.04.052
2. Lloyd-Jones DM, Braun LT, Ndumele CE, Smith Jr SD, Sperling LS, Virani SS, et al. Use of risk assessment tools to guide decisionmaking in the primary prevention of atherosclerotic
cardiovascular disease. Circulation 2019;139:e1162–77. https://doi.org/10.1161/CIR.0000000000000638
3. Cui J. Overview of risk prediction models in cardiovascular disease research.
Ann Epidemiol 2009;19:711-7.
https://doi.org/10.1016/j.annepidem.2009.05.005
4. Elosua R. Cardiovascular risk functions: usefulness and limitations. Rev Esp Cardiol (Engl
Ed) 2014; 67:77-9.
https://doi.org/10.1016/j.rec.2013.09.012
5. Verma KP, Inouye M, Meikle PJ, Nicholls SJ, Carrington MJ, Marwick TH, et al. New Cardiovascular Risk Assessment
Techniques for Primary Prevention: JACC Review Topic of the Week. J Am Coll Cardiol 2022; 80:373-87. https://doi.org/10.1016/j.jacc.2022.05.015
6. Nambi
V, Chambless L, Folsom AR, He M, Hu Y, Mosley T, et
al. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: the ARIC (Atherosclerosis
Risk In Communities) study. J Am Coll Cardiol 2010;55:1600-7. http://doi.org/cx9xd9
7. Nicolaides AN, Panayiotou AG, Griffin
MG, Tyllis T, Bond D, Georgiou N, et al. Arterial Ultrasound Testing to Predict
Atherosclerotic Cardiovascular Events. J Am Coll Cardiol
2022; 79:1969-82. https://doi.org/10.1016/j.jacc.2022.03.352
8. Budoff
MJ, Young R, Burke G, Carr JJ, Detrano RC, Folsom AR,
et al. Ten-year association of coronary artery calcium with atherosclerotic
cardiovascular disease (ASCVD) events: the multi-ethnic study of atherosclerosis (MESA). Eur Heart J 2018; 39:2401-08. https://doi.org/10.1093/eurheartj/ehy217
9. Abuzaid
A, Saad M, Addoumieh A, Ha
LD, Elbadawi A, Mahmoud AN, et al. Coronary artery calcium score and risk of
cardiovascular events without
established coronary artery disease: a systematic review and meta-analysis. Coron Artery Dis 2021; 32:317-28. http://dx.doi.org/10.1097/MCA.0000000000000974
10. Jawi
MM, Frohlich J, Chan SY. Lipoprotein(a) the Insurgent: A New Insight into the Structure, Function, Metabolism, Pathogenicity,
and Medications Affecting Lipoprotein(a) Molecule. J Lipids. 2020;2020:3491764. https://doi.org/10.1155/2020/3491764
11. Grundy SM, Stone NJ, Bailey AL,
Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/ AGS/APhA/ASPC/NLA/PCNA Guideline
on the Management of Blood
Cholesterol: A Report of the American College of Cardiology/ American Heart Association Task Force on Clinical Practice
Guidelines. Circulation 2019;139:e1082-e1143. https://doi.org/10.1161/CIR.0000000000000625
12. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of
low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 1972;18:499-502.
13. Levey
AS, Stevens LA. Estimating GFR using the CKD Epidemiology Collaboration (CKD-EPI) creatinine equation: More accurate GFR estimates, lower CKD prevalence
estimates, and better risk predictions. Am J Kidney 55:622-7. Am J Kidney Dis.2010;55:622-7. https://doi.org/10.1053/j.ajkd.2010.02.337
14. Visseren
FLJ, Mach F, Smulders YM, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice.
Eur Heart J. 2021;42:3227–37. https://doi.org/10.1093/eurjpc/zwab154
15. Sociedad Argentina de
Cardiología. Área de Consensos y Normas. Uso
apropiado de estatinas en Argentina: documento de
posición. Rev Argent Cardiol 2018;86(Sup.1):1-13.
16. Lloyd-Jones DM, Morris PB, Ballantyne CM, Birtcher KK, Covington
AM, DePalma SM, et al. 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin
Therapies for LDL-Cholesterol
Lowering in the Management of Atherosclerotic
Cardiovascular Disease Risk: A Report of the American College
of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol 2022;80:1366-418. https://doi.org/10.1016/j.jacc.2022.07.006
17. Kronenberg
F, Mora S, Stroes ESG, Ference
BA, Arsenault BJ, Berglund
L, et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis
Society consensus statement. Eur Heart J 2022;43:3925-46. https://doi.org/10.1093/eurheartj/ehac361
18. Davidson L, Wilcox J, Kim D, Benton S, Fredi J, Vaughan D. Clinical
features of precocious acute coronary syndrome. Am J Med 2014;127:140-4. https://doi.org/10.1016/j.amjmed.2013.09.025
19. Liu Q, Shi RJ, Zhang YM, Cheng YH, Yang BS, Zhang YK, et al. Risk factors,
clinical features, and outcomes of premature acute
myocardial infarction. Front Cardiovasc Med 2022;9:1012095. https://doi.org/10.3389/fcvm.2022.1012095
20. Razavi
AC, Mortensen MB, Blaha MJ, Dzaye
O. Coronary artery calcium testing
in young adults. Curr Opin Cardiol 2023;38:32-8. https://doi.org/10.1097/HCO.0000000000001006
21. Reese JA, Roman MJ, Deen JF, Ali T, Cole SA, Devereux RB, et al. Subclinical
atherosclerosis in adolescents and young adults and the risk of cardiovascular
disease: The Strong Heart Family Study (SHFS. Nutr Metab Cardiovasc Dis 2022;32:1863-71. https://doi.org/10.1016/j.numecd.2022.04.024
22. Javaid
A, Mitchell JD, Villines TC. Predictors
of coronary artery calcium and long-term risks of death, myocardial infarction, and
stroke in young adults. J Am Heart Assoc 2021;10(22): e022513. https://doi.org/10.1161/JAHA.121.022513
23. Coll
B, Betriu A, Feinstein SB, Valdivielso
JM, Zamorano JL, Fernández E. The role of carotid
ultrasound in assessing carotid atherosclerosis in individuals at low-to-intermediate
cardiovascular risk. Rev Esp Cardiol (Engl
Ed) 2013;66:929-34. https://doi.org/10.1016/j.rec.2013.05.030
24. Masson W, Lobo M, Huerín M, Molinero
G, Manente D, Pángaro M, et al. Estratificación del riesgo cardiovascular
con diferentes puntajes de riesgo en
prevención primaria y sus implicaciones en la
indicación de estatinas. Rev Argent Cardiol 2014;82:480-6. http://dx.doi.org/10.7775/rac.es.v82.i6.4527
25. Lluberas N. Score de calcio coronario
en la estratificación de riesgo cardiovascular. Rev Urug Cardiol
2019;34:341-8. https://doi.org/10.29277/cardio.34.3.23
26. Bea AM, Civeira
F, Jarauta E, Lamiquiz-Moneo
I, Pérez-Calahorra S, Marco-Benedí V, et al. Association Between the Presence of Carotid Artery Plaque and
Cardiovascular Events in Patients With
Genetic Hypercholesterolemia. Rev Esp
Cardiol (Engl Ed). 2017;70:551-8. https://doi.org/10.1016/j.rec.2017.01.023
27. Gallo A, Pérez de Isla L, Charrière S, Vimont A, Alonso R,
Muñiz-Grijalvo O, et al. The Added Value of Coronary Calcium Score in Predicting Cardiovascular Events in
Familial Hypercholesterolemia. JACC Cardiovasc Imaging 2021;14:2414-24. https://doi. org/10.1016/j.jcmg.2021.06.011
28. Alonso R, Andrés E, Mata N,
Fuentes-Jiménez F, Badimón L, López-Miranda J, et
al. Lipoprotein(a) levels in familial hypercholesterolemia: an important predictor of cardiovascular disease independent of the type of LDL receptor mutation. J Am Coll
Cardiol. 2014;63:1982-9. https://doi.org/10.1016/j.jacc.2014.01.063
29. Mattina A, Giammanco A, Giral P, Rosenbaum D, Carrié A, Cluzel P, et al. Polyvascular
subclinical atherosclerosis in familial hypercholesterolemia: The role of
cholesterol burden and gender. Nutr Metab Cardiovasc Dis. 2019;29:1068-76. https://doi.org/10.1016/j. numecd.2019.06.015
30. Gepner
AD, Young R, Delaney JA, Tattersall MC, Blaha MJ,
Post WS, et al. Comparison of coronary artery calcium presence, carotid plaque presence, and carotid intima-media
thickness for cardiovascular disease prediction in the Multi-Ethnic Study of Atherosclerosis. Circ Cardiovasc Imaging
2015;8:e002262. https://doi.org/10.1161/CIRCIMAGING.114.002262
31. Siniawski
D, Masson W, Bluro I, Falconi M, Pérez De Arenaza D, De Stefano L, et al. Precisión
diagnóstica del espesor íntima-media carotídeo para la detección de aterosclerosis coronaria.
Utilidad en la práctica clínica. Rev
Argent Cardiol 2013;81:136-43.
http://dx.doi. org/10.7775/rac.es.v81.i2.2114
32. Moreyra
E Jr, Moreyra C, Tibaldi MA, Crespo F, Arias V, Lepori AJ, et al. Concordance and prevalence of subclinical atherosclerosis in different vascular territories. Vascular 2020;28:285-294. http://dx.doi.org/10.1177/1708538119894178
33. Forbes CA, Quek
RG, Deshpande S, Worthy G, Wolff R, Stirk L, et al. The relationship between Lp(a) and CVD outcomes:
a systematic review. Lipids Health Dis 2016;15:95. https://doi.org/10.1186/s12944-016-0258-8
34. Saleheen D, Haycock PC, Zhao W, Rasheed
A, Taleb A, Imran
A, et al. Apolipoprotein(a) isoform size,
lipoprotein(a) concentration, and
coronary artery disease: A mendelian randomisation analysis. Lancet Diabetes
Endocrinol 2017;5:524-33. https://doi.org/10.1016/S2213-8587(17)30088-8
35. Kamstrup
PR. Lipoprotein(a) and Cardiovascular Disease. Clin Chem 2021;67:154-66. https://doi.org/10.1093/clinchem/hvaa247
36. Muhlestein
JB, Knowlton KU, Le VT, Lappe DL, May HT, Min DB, et al. Coronary Artery Calcium Versus
Pooled Cohort Equations Score for Primary Prevention Guidance: Randomized Feasibility Trial. JACC Cardiovasc
Imaging 2022;15:843-55. https://doi.org/10.1016/j.jcmg.2021.11.006
37. Effectiveness of a Proactive Cardiovascular Primary Prevention Strategy, With or Without the Use of
Coronary Calcium Screening, in Preventing
Future Major Adverse Cardiac Events (CorCal). Acceso el 11/01/2023 desde: https://clinicaltrials.gov/ct2/show/NCT03439267