ORIGINAL ARTICLE
Behavior of Retrograde Conduction Time at Supraventricular Tachycardia Induction and its Role in Differential Diagnosis
Comportamiento del tiempo de conducción retrógrada al momento de la inducción de las taquicardias supraventriculares y su rol en el diagnóstico diferencial
Claudio HadidMTSAC1,2,3,4, Leonardo
CelanoMTSAC 1,2, Darío Di ToroMTSAC 1,2, Edgar Antezana-Chávez1, Sebastián Gallino3,
Gustavo Iralde4, Leonardo Atea5,
Sergio Gonzalez6, Sebastián Maldonado7, Carlos LabadetMTSAC1,2
1 Hospital General de Agudos Dr. Cosme Argerich.
Autonomous City of Buenos Aires, Argentina.
2 Hospital Universitario CEMIC.
Autonomous City of Buenos Aires,
Argentina.
3 Sanatorio Garat. Concordia, Entre Ríos, Argentina.
4 Cardiovascular Chivilcoy. Chivilcoy, Buenos Aires, Argentina.
5 Sanatorio del Salvador.
Córdoba, Argentina.
6 Instituto de Cardiología. Tucumán,
Argentina.
7 Hospital
Prof. Dr. Juan Garrahan. Autonomous City of Buenos Aires, Argentina.
Address for reprints: Claudio Hadid. Pi y Margal 750, CABA. Email:
claudio.hadid@gmail.com
Part of the present
work’s data has already been published in: Hadid, C., Celano,
L., Di Toro, D. et al. Variability of the VA interval at tachycardia induction:
a simple method to differentiate orthodromic reciprocating tachycardia
from atypical atrioventricular nodal reentrant
tachycardia. J Interv Card Electrophysiol (2022). https://doi.org/10.1007/s10840-022-01376-w
Rev Argent Cardiol
2023;91:110-117. http://dx.doi.org/10.7775/rac.v91.i2.20611
ABSTRACT
Background: Differential diagnosis between orthodromic
reentrant tachycardia (ORT) and atypical nodal reentrant tachycardia (ANRT) can be challenging. Our hypothesis
was that ANRT presents more variability in retrograde conduction time at
tachycardia onset than ORT.
Objectives: The objectives of this study were to assess retrograde
conduction time variability at the start of tachycardia in ANRT and ORT, and postulate a new diagnostic tool to differentiate these two types of arrhythmias.
Methods: The ventriculoatrial (VA)
interval of the first beats after tachycardia induction was measured until
stabilization. The difference between
the maximum and minimum VA interval was defined as delta VA (∆VA), and
the number of beats needed for VA interval stabilization was also assessed.
Atrial tachycardias were excluded.
Results: In a total of 101 patients included in the study, ORT was
diagnosed in 64 patients and ANRT in 37. ∆VA interval was 0 (interquartile range [IQR] 0-5)
milliseconds (ms) in ORT vs. 40 (21-55) ms in ANRT (p <0.001). The VA interval significantly
stabilized earlier in ORT (1.5 [1-3] beats) than in ANRT (5 [4-7] beats)
(p<0.001). A ∆VA <10 ms diagnosed ORT
with 100% sensitivity, specificity, and positive and negative predictive values. Ventriculoatrial interval stabilization in less than 3 beats predicted ORT with
good diagnostic accuracy. The results were similar considering only accessory septal pathways. Typical NRTs presented an intermediate variation.
Conclusion: Presence of ∆VA <10 ms
is a simple criterion that accurately differentiates ORT from ANRT,
independently of the accessory pathway localization.
Key words: Tachycardia, Supraventricular - Tachycardia, Atrioventricular Nodal Reentry - Tachycardia, Ectopic Junctional
RESUMEN
Antecedentes: el diagnóstico diferencial entre
la taquicardia reentrante ortodrómica (TRO) y la taquicardia por reentrada
nodal atípica (TRNa)
puede ser dificultoso. Nuestra hipótesis es que las TRNa
tienen más variabilidad en el tiempo de conducción retrógrada al comienzo de la taquicardia que las TRO.
Objetivos: nuestros objetivos fueron evaluar
la variabilidad en el tiempo de conducción retrógrada al inicio de la
taquicardia en TRNa y TRO, y proponer una nueva herramienta diagnóstica para diferenciar estas dos arritmias.
Métodos: se midió el intervalo
ventrículo-auricular (VA) de los primeros latidos tras la inducción de la
taquicardia, hasta su estabilización. La diferencia entre el intervalo VA
máximo y el mínimo se definió como delta VA (∆VA). También contamos el
número de latidos necesarios
para que se estabilice el intervalo VA. Se excluyeron las taquicardias auriculares.
Resultados: se incluyeron 101 pacientes. Se diagnosticó TRO en 64 pacientes y TRNa en 37. El ∆VA
fue 0 (rango intercuartílico, RIC, 0-5) milisegundos (ms) en la TRO frente
a 40 (21-55) ms en la TRNa (p <0,001). El intervalo VA se estabilizó significativamente antes en la TRO (1,5 [1-3] latidos) que en
la TRNa (5 [4-7] latidos; p <0,001). Un ∆VA
<10 ms diagnosticó TRO con 100% de sensibilidad,
especificidad y valores predictivos positivo y negativo. La estabilización del
intervalo VA en menos de 3 latidos predijo TRO
con buena precisión diagnóstica. Los resultados fueron similares considerando
sólo vías accesorias septales. Las TRN típicas tuvieron
una variación intermedia.
Conclusión: un ∆VA
< 10 ms es un criterio simple, que distingue
con precisión la TRO de la TRNa, independientemente de la localización de la vía accesoria.
Palabras clave: Taquicardia Supraventricular - Taquicardia por Reentrada en el Nodo Atrioventricular - Taquicardia Ectópica de Unión
Received: 09/12/2022
Accepted: 02/17/2023
INTRODUCTION
Regardless several criteria have been described, the differential diagnosis between orthodromic reentrant tachycardia
(ORT) through an occult accessory pathway (AP) and atypical intranodal
reentrant tachycardia (ANRT) can be challenging. (1-15) The usefulness of
these techniques usually depends on certain factors, such as sustained
tachycardia and the distance from the
stimulation site to the tachycardia circuit, as well as on certain conditions, as an adequate
bundle of His recording or capture, and that the tachycardia is not interrupted by stimulation
maneuvers or post- stimulation
interval correction due to atrioventricular (AV) nodal delay caused after
entrainment from the right ventricle
(RV).
Conceptually, these techniques are based on localization,
size and distance of the circuit to certain structures as the His bundle,
the apex, or basal portions
of the RV, and have not been focused
on the electrophysiological
components of each circuit. ORT and ANRT use AV nodal tissue as antegrade
limb of the tachycardia
circuit. However, this is not the case for the retrograde limb. Although retrograde conduction runs by an AP in ORT, it travels through
a slower pathway
of the AV node in ANRT (both
in the slow-slow as in the fast-slow forms). Therefore, retrograde conduction properties are different in ORT, typically
independent of heart rate (HR), from typically decremental or dependent on HR in ANRT.
The abrupt change
in HR that occurs at tachycardia onset causes changes in the conduction properties and refractoriness of the involved tissues. Our hypothesis is that this difference in retrograde conduction between ORT and ANRT can be better evidenced during
tachycardia induction, in terms of greater retrograde conduction time variability in the first beats of ANRT than in those of ORT. The objectives
of the study were to systematically analyze
and compare retrograde conduction time variability at the start of ANRT and ORT, and find a cut-off
value that constitutes a new diagnostic tool to differentiate between
these two arrhythmias. Additionally, we included a few patients with ORT mediated
via a decremental conduction AP and a group
of patients with typical NRT (tNRT). The analysis
of tNRT was not carried out for diagnostic purposes,
but with the objective of performing a pathophysiological description of retrograde conduction behavior in different
types of paroxysmal
supraventricular tachycardia (SVT).
METHODS
Study population
Patients with SVT referred for electrophysiological study
were included in the analysis.
Irregular tachycardia, preexcitation during sinus rhythm,
atrial tachycardia, two coexistent mechanisms of arrythmia (e.g. ANRT with AP) and previous
ablation were considered exclusion criteria. Since
bundle branch block prolongs
the ventriculoatrial (VA) in ORTs that use an ipsilateral
AP, patients with transient bundle branch block after induction were also excluded.
No patient had structural
heart disease. The study was approved by the Ethics and Research Committees of
the participating centers.
Electrophysiological
study
After obtaining the informed consent, an electrophysiological
study was performed in fasting patients under local anesthesia, without
sedation. All antiarrhythmic drugs were discontinued for at least 5 half-lives
before the study. Surface and intracavitary electrophysiological tracings were recorded
in a digital polygraph, and blindly electronically analyzed at 200 mm/s by two electrophysiologists. In these conditions, the expected measurement margin of error
of intracardiac intervals
is considered to be ±5 ms at 100 mm/s and less at greater speeds (±1 ms at 400 mm/s). (16)
The diagnosis of NRT and ORT was performed according to
standard electrophysiological criteria, (2,5-15,17-19) and the ablation outcome. A fast-slow ANRT was considered when the AH interval was <180 ms and the AH/HA ratio
<1 during tachycardia. (20-22) The criteria for a successful ablation were: no tachycardia inducibility,
elimination of AP conduction in ORT and exclusion of sustained conduction
via the slow pathway in ANRT. Supraventricular tachycardia was induced
through programmed atrial or ventricular stimulation.
Isoproterenol was administered if tachycardia
was non-inducible or not sustained.
Variability of retrograde conduction time was measured to evaluate the VA intervals of the first
beats after tachycardia induction, until this interval was stabilized. A stable
VA interval was assumed when its duration
was not modified
for 3 consecutive beats and was equal to the VA interval of the established tachycardia. The VA interval
was measured from the beginning of the QRS interval in a surface
lead to a bipolar septal atrial electrogram (usually proximal coronary sinus). We preferred
coronary sinus recordings since the
ventricular electrogram is far field and low voltage,
and the coronary sinus recording
allows a clear identification of atrial
electrogram onset and its stable position. Maximum and minimum VA interval (VAmax and VAmin) were identified
and ∆VA was calculated for each type of tachycardia (∆VA=VAmax
– VAmin), independently of the stable VA interval.
The number of beats necessary for VA interval stabilization was also assessed.
Statistical analysis
Discrete variables were expressed as percentages and continuous
variables as mean ± standard deviation or median and interquartile range (IQR 25-75) according to their distribution.
The chi-square test or Fisher’s exact test was used for discrete variables and the Mann-Whitney U test for continuous
variables. Sensitivity, specificity, and positive and negative predictive
values (PPV, NPV) were calculated using the electrophysiological
study diagnosis as gold standard. The area under
the ROC curve
(AUC) for ∆VA and the number
of beats needed for VA stabilization variables
was calculated to
differentiate between ORT and ANRT. Youden’s J
statistic was considered to find the
best cut-off point for these variables.
(23) A p value <0.05 was considered as statistically significant. IBMSPSS v.26 (Armonk, NY,
USA) was used to perform the analyses.
RESULTS
A total of 156 patients (73 men) with median age 46 (29-65)
years were included
in the study. Among them,
37 patients were diagnosed with ANRT and 64 had ORT via a classical occult fast conduction AP (Kent bundle), with septal (n=33), left lateral
(n=30) or right lateral (n=1)
localization. Six patients were also included
with ORT via a decremental conduction AP (Coumel type)
which were separately analyzed. The remaining 49 cases formed the group with tNRT.
ANRT analysis
All ANRTs had some degree of variability in the time of retrograde conduction, i.e. no ANRT exhibited
a fixed VA interval. Median
∆VA was 40 (21-55) ms and the VA interval stabilized in 5 (4-7) beats (Figure 1).
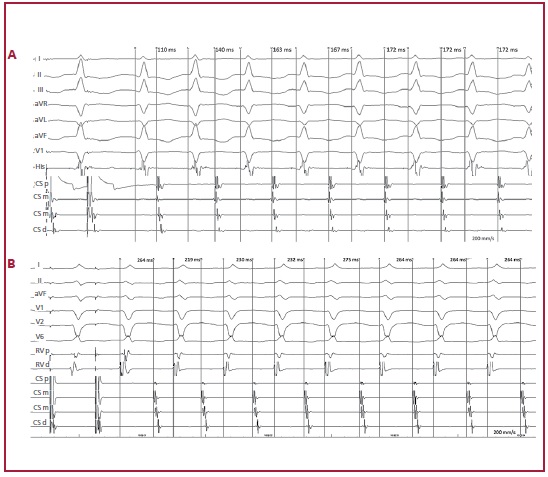
Fig. 1. ANRT induction in 2 different
patients. A: Induction by programmed atrial
stimulation. The VA interval stabilizes in the 5th beat and ∆VA is 62 ms
(maximum VA interval: 172 ms; minimum VA
interval: 110 ms). The VA interval was measured from the beginning
of the QRS complex in V1 to
the atrial electrogram
in the proximal coronary
sinus. The intracavitary recordings are bundle of His and proximal
(p), medial (m) and
distal (d) coronary sinus (CS). B: Induction by programmed atrial stimulation. The VA interval stabilizes in the 6th beat and ∆VA is 56 ms (maximum VA interval: 275 ms; minimum VA interval: 219
ms). The VA interval was measured from the beginning of the QRS complex in V2 to the atrial
electrogram
in the medial coronary sinus. The intracavitary recordings were proximal (p) and distal right ventricle (RV) and proximal
(p), medial (m) and distal (d) coronary sinus (CS).
ANRT: atypical
nodal reentrant tachycardia; VA: ventriculoatrial
Comparison with ORT
Thirty-two (50%) ORTs displayed no variability in the VA interval (Figure 2), exhibiting a ∆VA interval of 0 (0-5) ms, significantly lower than in ANRT (p<0.001). The
VA interval stabilized in 1.5 (1-3) beats, significantly before than in ANRT (p<0.001) (Table 1). These findings
were similar in septal
and free wall APs.
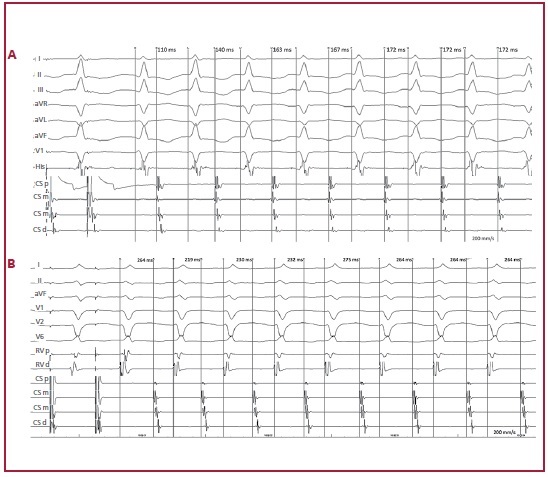
Fig.
2. ORT induction using a septal accessory
pathway in 2 different patients. A: Induction by atrial extra stimulus over sensed rhythm.
Tachycardia has a fixed VA interval from
the first beat. ∆VA is 0 ms. The VA interval was measured
from the beginning of the V2 complex
to the atrial electrogram in the proximal
coronary sinus. Intracavitary recordings are proximal (p), medial (m) and distal (d) coronary
sinus (CS) and proximal
(p) and distal (d) His bundle. B: Induction by programmed atrial
stimulation. Tachycardia has a fixed VA interval from the first beat. ∆VA is 0 ms. The VA interval was measured
from the beginning of the V2 complex
to the atrial electrogram
in the proximal coronary sinus. Intracavitary
recordings are His bundle and proximal
(p), medial (m) and distal (d) coronary sinus (CS).
ORT: Orthodromic reentrant
tachycardia. VA: ventriculoatrial
Table 1. VA interval variability in ORT and ANRT
|
|
ORT
(n=64)
|
ANRT
(n=37)
|
|
ΔVA (ms)
|
0 (0-5)
|
40 (21-55) *
|
|
Number of beats
|
1.5 (1-3)
|
5 (4-7) *
|
|
ΔVA <10 ms
|
64/64 (100%)
|
0/37 (0%) *
|
|
Beats <3
|
41/64 (64.1%)
|
2/37 (5.4%) *
|
* p <0.001 for all comparisons.
∆VA: Difference between maximum and minimum VA interval; Beats <3:
patients with stable VA interval in <3 beats; Number of beats: necessary number of beats for VA interval stabilization; ANRT: Atypical nodal reentrant
tachycardia; ORT: Orthodromic reentrant tachycardia;
VA: ventriculoatrial
No ORT had ∆VA10 ms. As shown in Figure 3, ∆VA <10 ms differentiated ORT from ANRT with
100% sensitivity, specificity, PPV and NPV. Stabilization of the VA
interval in less than 3 beats identified ORT with 64.1% sensitivity, 94.6% specificity, 95.3% PPV, 60.3% NPV and AUC of 0.895 (Table 2).
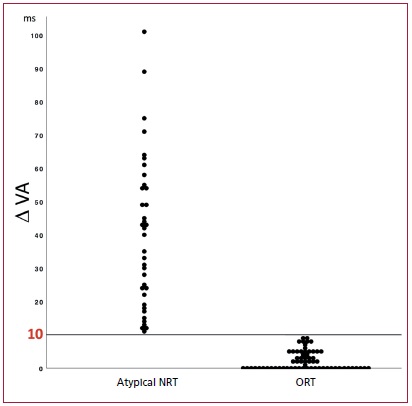
Fig. 3. The scatter diagram shows individual ∆VA in ANRT and ORT. The 10 ms line represents the cut-off value to differentiate between these two arrhythmia
mechanisms.
Atypical
NRT. Atypical nodal reentrant tachycardia; ORT: Orthodromic reentrant tachycardia
Table 2. Diagnostic yield of VA
interval variability to differentiate ORT from ANRT
|
|
Sensitivity
|
Specificity
|
PPV
|
VPN
|
ABC
|
|
ORT
vs. ANRT
|
|
ΔVA <10 ms
|
100%
|
100%
|
100%
|
100%
|
1
|
|
Beats
<3
|
64.1%
(52-76%)
|
94.6%
(87-100%)
|
95.3%
(89‑100%)
|
60.3%
(48-73%)
|
0.895
(0.836-0.954)
|
|
ORT (septal
accessory pathways) vs. ANRT
|
|
ΔVA
<10 ms
|
100%
|
100%
|
100%
|
100%
|
1
|
|
Beats <3
|
54-5%
(38-72%)
|
94-6%
(87-100%)
|
90%
(77-100%)
|
70%
(57-83%)
|
0.857
(0.771-0.954)
|
|
|
|
|
|
|
|
|
∆VA: Difference between
maximum and minimum
VA interval; ANRT:
Atypical nodal reentrant
tachycardia; AUC:
Area under the ROC curve; Beats <3: patients with stable VA interval in
<3 beats; NPV: Negative predictive value; ORT: Orthodromic reentrant tachycardia; PPV: Positive predictive value.
Values between parentheses represent 95% confidence interval. VA: ventriculoatrial
The comparison between
ANRT and ORT via septal AP
(n=33) presented similar results. A ∆VA <10 ms identified ORT with 100% sensitivity, specificity, PPV and NPV.
Stabilization of the VA interval in less than
3 beats predicted ORT with 54.5% sensitivity,
94.6% specificity, 90% PPV, 70% NPV and AUC of 0.857 (Table 2).
Subgroup of patients
with decremental conduction AP
In the six patients with decremental conduction AP, ∆VA was significantly lower (15 [5-20] ms; p=0.006) than in patients
with ANRT, but the
VA interval was stabilized in a
similar number of beats (4 [3-7]; p=0.481).
A ∆VA <20 ms identified these patients with 83.3% sensitivity, 74.2% specificity, 38.5% PPV, 95.8% NPV and AUC of 0.844. The ORTs via decremental pathways were compared
with fast-slow ANRT, as they present with SVT with long RP. A ∆VA<20 ms predicted ORT mediated
by decremental conduction pathways with 83.3% sensitivity, 73.3% specificity, 55.6% PPV, 91.7% NPV and AUC of 0.856.
Previous studies
Variability in the AV relation during tachycardia has been consistently associated with atrial
tachycardia. (24,25) This can occur spontaneously or in response to stimulation aneuvers. Effectively, this criterion has been used to differentiate atrial
tachycardia from NRT in which atrial
activation is assumed as “associated” to ventricular activation. (1,5,24-26) This assumption
has been considered for ORT throughout all publications on SVT.
A recent study showed changes in retrograde conduction time after fast-slow ANRT induction. (27) The authors reported shortening of the first HA interval compared
with the HA interval of the established tachycardia. We analyzed all
the VA intervals since the start of
tachycardia until it attained a stable duration for 3 consecutive beats and included
not only fast-slow ANRT but all ANRTs, as well as ORTs. As previously mentioned, VA interval variability in this study did not
exhibit a uniform pattern (incremental or decremental).
In an analysis
of 411 patients with typical
and atypical NRT, Taniguchi et el. reported variations in the P-QRS relation during tachycardia. (28) The authors defined variation of the P-QRS relation
during tachycardia as a change
in the AH and HA intervals
>20 ms, together
with a change in the AH/HA ratio.
This phenomenon was found in 19 % of cases with ANRT at tachycardia onset (only 3 patients) during a Wenckebach AV or 2:1 block, or at the end of spontaneous or secondary to adenosine administration tachycardia. This study did not include patients
with ORT. VA interval variability at tachycardia induction had never been used as a criterion
to distinguish ANRT from ORT. We analyzed
the VA relation only at tachycardia induction, both in ANRT as in ORT, and found that all ANRTs had some degree of variability compared with only 50% in ORTs. ∆VA was <10 ms in
all ORTs and in none of the ANRTs.
This is an easily applicable criterion without the usual limitations of the commonly used
electrophysiological maneuvers (e.g. non-sustained tachycardia, termination during entrainment attempts, loss of capture during
stimulation, or His bundle inadequate recording or capture). It can be
evaluated measuring the initial VA
intervals of tachycardia, without additional
maneuvers. The only requisite that must be fulfilled is tachycardia induction.
The study of Obeyesekere et al. also focused
on tachycardia induction
to differentiate ORT from
ANRT. They proposed applying during induction criteria that are used after
entrainment (post-stimulation interval and stimulus-atrium interval), to manage non-sustained tachycardias. (29) However, the marked variability of the initial VA
intervals in our study (VA=40 [21-55] ms in ANRT) may lead to a false
diagnosis with this maneuver. Moreover, the criteria
postulated by Obeyesekere is limited to tachycardias induced from the ventricle. Our findings were similar in tachycardias
induced by atrial and ventricular stimulation. The fact that an adequate
diagnosis was performed in a median
of 5 beats since tachycardia induction, suggests the potential usefulness of VA interval
variability in non-sustained SVT.
The value of ∆VA for ORT diagnosis is independent of AP localization. The usefulness of
many diagnostic criteria described is
lower in the presence of left lateral AP. (4,30-32)
Possible mechanisms
As previously mentioned, the retrograde limb of the tachycardia circuit has different
properties in ORT and ANRT. The refractory period is longer
in the first tachycardia beat and progressively shortens when this starts. In this scenario,
retrograde conduction via a slow nodal pathway can be less uniform
and show different conduction times from the one occurring via an AP with all-or-none conduction. (33,34)
Another possible explanation for VA interval
variability in ANRT is the occult penetration of the extra stimulus
that initiates the tachycardia, which
results in different conduction
times and degrees of refractoriness in the rest of the circuit. Occult
conduction between fast and slow
pathways was demonstrated in patients with dual AV nodal physiology. (35,36)
Lastly, a final common superior pathway could be the seat of retrograde conduction
changes. (37,38) Since tNRT had lower VA variability
than ANRT, a different behavior of the final common pathway should be assumed in these two situations.
Limitations
Although ∆VA showed excellent diagnostic accuracy,
it has some limitations. Irregular tachycardias were not included
to avoid the influence of cycle length or antegrade
conduction changes on retrograde conduction
time. The value of our criterion lies in the identification of small
changes in the initial VA intervals of a regular
tachycardia. Tachycardias with transient bundle branch
block were also excluded. The results of the present
study do not apply in these two situations.
In addition, atrial tachycardias
were also excluded from the study.
Since these tachycardias may have VA interval variation, they must be ruled out
by means of other criteria before performing the ANRT diagnosis.
CONCLUSION
Retrograde conduction time after SVT induction is significantly
more variable (in terms of ∆VA and the
necessary number of beats to reach VA interval stabilization) in ARNT
than in ORT. A ∆VA <10 ms distinguished ORT
from ANRT with 100% sensitivity and specificity.
We present a new method, simple and accurate, which does not require additional
maneuvers to tachycardia induction,
and that should be employed to
perform the differential diagnosis between ANRT and ORT, independently of AP localization.
Conflicts of interest
None declared.
(See authors' conflict of interests
forms on the web/Additional material.)
Funding
None.
 https://creativecommons.org/licenses/by-nc-sa/4.0/
https://creativecommons.org/licenses/by-nc-sa/4.0/
©Revista Argentina de Cardiología
REFERENCES
1. Kadish
AH, Morady F. The response of paroxysmal
supraventricular tachycardia to overdrive atrial and ventricular pacing: can it
help determine the tachycardia
mechanism? J Cardiovasc
Electrophysiol 1993;4:239-52. https://doi.org/10.1111/j.1540-8167.1993.tb01227.x
2. Ormaetxe
JM, Almendral J, Arenal A, Martínez-Alday JD, Pastor
A, Villacastín JP,
et al. Ventricular fusion during resetting and entrainment of orthodromic supraventricular tachycardia involving septal accessory
pathways. Implications
for the differential diagnosis with atrioventricular nodal
reentry. Circulation 1993;88:2623-31. https://doi.org/10.1161/01.CIR.88.6.2623
3. Martínez-Alday JD, Almendral J, Arenal A, Ormaetxe JM, Pastor A,
Villacastín JP,
et al. Identification of concealed posteroseptal
Kent pathways by comparison of ventriculoatrial intervals from apical and posterobasal right ventricular
sites. Circulation 1994;89:1060-7. https://doi.org/10.1161/01.CIR.89.3.1060
4. Hirao
K, Otomo K, Wang X, Beckman KJ, McClelland JH, Widman L, et al. Para-Hisian
pacing. A new method for differentiating retrograde
conduction over an accessory AV pathway from conduction over the AV node. Circulation 1996;94:1027-35. https://doi.org/10.1161/01.CIR.94.5.1027
5. Knight BP, Ebinger M, Oral H, Kim MH, Sticherling C, Pelosi F, et al. Diagnostic value of tachycardia features and pacing
maneuvers during paroxysmal supraventricular tachycardia. J
Am Coll Cardiol 2000;36:574-82. https://doi.org/10.1016/S0735-1097(00)00770-1
6. Michaud GF, Tada H, Chough S,
Baker R, Wasmer K, Sticherling C, et al. Differentiation of atypical atrioventricular node re-entrant tachycardia
from orthodromic reciprocating tachycardia
using a septal
accessory pathway by the response to ventricular pacing. J Am Coll
Cardiol 2001;38:1163-7. https://doi.org/10.1016/S0735-1097(01)01480-2
7. Reddy VY, Jongnarangsin
K, Albert CM, Sabbour H, Keane. D, Mela. T, et al. Para-Hisian entrainment: a novel pacing maneuver to
differentiate orthodromic atrioventricular
reentrant tachycardia from atrioventricular nodal
reentrant tachycardia. J. Cardiovasc. Electrophysiol. 2003;14:1321-8. https://doi.org/10.1046/j.1540-8167.2003.03239.x
8. González-Torrecilla E, Arenal A, Atienza F, Osca J, García- Fernández
J, Puchol
A, et al. First postpacing interval after
tachycardia entrainment with correction for atrioventricular node delay:
a simple maneuver
for differential diagnosis
of atrioventricular nodal reentrant
tachycardias
versus orthodromic reciprocating tachycardias. Heart Rhythm 2006;3:674-9. https://doi.org/10.1016/j.hrthm.2006.02.019
9. González-Torrecilla E, Almendral
J, García-Fernández FJ, Arias MA,
Arenal A, Atienza F, et al. Differences in ventriculoatrial in- tervals during entrainment
and tachycardia: a simpler method for distinguishing paroxysmal supraventricular tachycardia with long ventriculoatrial intervals. J Cardiovasc
Electrophysiol 2011;22:915- 21. https://doi.org/10.1111/j.1540-8167.2011.02020.x
10. Segal OR, Gula
LJ, Skanes AC, Krahn AD,
Yee R, Klein GJ. Differential ventricular entrainment: a maneuver to
differentiate AV node reentrant tachycardia from orthodromic
reciprocating tachycardia. Heart Rhythm 2009;6:493–500. https://doi.org/10.1016/j. hrthm.2008.12.033
11. Padanilam
BJ, Ahmed AS, Clark BA, Gilge JL, Patel PJ, Prystowsky EN, et al. Differentiating
Atrioventricular Reentry Tachy- cardia and Atrioventricular Node Reentry Tachycardia Using Premature His Bundle Complexes. Circ. Arrhythm. Electrophysiol. 2020;13:e007796. https://doi.org/10.1161/CIRCEP.119.007796
12. Miller JM, Rosenthal ME,
Gottlieb CD, Vassallo JA, Josephson ME. Usefulness of the delta HA interval to accurately distinguish atrioventricular nodal reentry from orthodromic septal bypass tract
tachycardias. Am. J. Cardiol. 1991;68:1037-44.
https://doi.org/10.1016/0002-9149(91)90492-4
13. Calvo D, Pérez D, Rubín J, García
D, Ávila P, Javier García-Fernández F, et al. Delta of the local ventriculo-atrial
intervals at the septal location to differentiate
tachycardia using septal accessory pathways
from atypical atrioventricular nodal re-entry. Europace 2018;20:1638-46. https://doi.org/10.1093/europace/eux368
14. Sellers TD, Gallagher JJ, Cope GD, Tonkin AM,
Wallace AG. Retrograde atrial preexcitation
following premature ventricular beats during
reciprocating tachycardia in the Wolff Parkinson White syndrome. Eur J Cardiol 1976;4:283-94. https://doi.org/10.1016/0002-9149(76)90600-7
15. Katritsis DG, Josephson ME. Differential diagnosis of regular, narrow QRS tachycardias.
Heart Rhythm 2015;12:1667-76. https://doi.org/10.1016/j.hrthm.2015.03.046
16. Josephson ME. Electrophysiologic investigation: general
concepts. En: Clinical Cardiac Electrophysiology. Techniques
and Interpretations. Third Edition. Philadelphia, PA: Lippincott Williams
& Wilkins, 2002:19–67.
17. Benditt DG, Pritchett EL, Smith WM, Gallagher JJ. Ventriculoatrial intervals: diagnostic use in paroxysmal supraven- tricular tachycardia. Ann Intern Med 1979;91:161-6. https://doi.org/10.7326/0003-4819-91-2-161
18. Katritsis
DG, Camm AJ. Atrioventricular nodal reentrant tachycardia. Circulation 2010;122:831-40. https://doi.org/10.1161/CIRCULATIONAHA.110.936591
19. Katritsis
DG, Josephson ME. Classification of electrophysiological types of atrioventricular nodal re-entrant tachycardia: a reappraisal. Europace 2013;15:1231-40. https://doi.org/10.1093/euro- pace/eut100
20. Heidbüchel H, Jackman WM. Characterization of subforms of AV
nodal reentrant tachycardia. Europace 2004;6:316-29. https://doi.org/10.1016/j.eupc.2004.03.004
21. Lockwood D, Nakagawa H, Jackman WM. Electrophysiologic characteristics
of atrioventriicular nodal reentrant tachycardia: implications
for reentrant circuits. In: Zipes DP, Jalife J (eds.). Cardiac Electrophysiology: From Cell to Bedside. 5th ed. Pennsylvania, PA: Saunders; 2009:615-45.
22. Gonzalez MD, Banchs JE, Moukabary T, Rivera J. Ablation of atrioventricular junctional tachycardias:
atrioventricular nodal reentry, variants and focal junctional
tachycardia. In: Huang SKS, Wood MA. Catheter Ablation of Cardiac Arrhythmias. 4th ed. Penn- sylvania, PA:
Elsevier; 2020:316-48. https://doi.org/10.1016/B978-0-323-52992-1.00021-1
23. Youden WJ. Index for rating diagnostic tests. Cancer 1950;3:32–35. https://doi.org/10.1002/1097-0142(1950)3:1<32::AID-CNCR2820030106>3.0.CO;2-3
24. Roberts-Thomson KC, Kistler PM, Kalman JM. Focal atrial tachycardia I: clinical features,
diagnosis, mechanisms, and ana-tomic location. Pacing Clin Electrophysiol 2006;29:643-52. https://doi.org/10.1111/j.1540-8159.2006.00413.x
25. Veenhuyzen GD, Quinn FR, Wilton SB, Clegg R, Mitchell LB. Diagnostic pacing maneuvers for supraventricular tachycardias: part 2. Pacing Clin.
Electrophysiol 2012;35:757-69. https://doi.org/10.1111/j.1540-8159.2012.03352.x
26. Maruyama M, Kobayashi Y, Miyauchi Y, Ino T, Atarashi H, Katoh T, et al. The VA relationship after differential atrial overdrive
pacing: a novel tool for the diagnosis of atrial tachycardia
in the electrophysiologic laboratory. J Cardiovasc Electrophysiol 2007;18:1127-33. https://doi.org/10.1111/j.1540-8167.2007.00928.x
27. Tamura S, Nakajima T, Iizuka T, Hasegawa H, Kobari T, Kurabayashi M, et al. Unique electrophysiological
properties of fast- slow atrioventricular nodal
reentrant tachycardia characterized by a shortening of retrograde conduction
time via a slow pathway manifested
during atrial induction. J Cardiovasc Electrophysiol 2020;31:1420-9. https://doi.org/10.1111/jce.14501
28. Taniguchi
Y, Yeh SJ,
Wen MS, Wang CC, Lin FC, Wu D. Variation of P-QRS relation during atrioventricular node reentry
tachycardia. J Am Coll Cardiol 1999;33:376-84. https://doi.org/10.1016/S0735-1097(98)00576-2
29. Obeyesekere
M, Gula LJ, Modi S,
Leong-Sit P, Angaran P, Mechulan A, et al. Tachycardia induction with ventricular extrastimuli differentiates atypical
atrioventricular nodal reentrant tachycardia from orthodromic reciprocating tachycardia. Heart Rhythm 2012;9:335-41. https://doi.org/10.1016/j.hrthm.2011.10.015
30. Singh DK, Viswanathan MN, Tanel RE, et
al. His overdrive pacing during supraventricular
tachycardia: a
novel maneuver for distinguishing atrioventricular
nodal reentrant tachycardia from atrioventricular reciprocating tachycardia. Heart Rhythm 2014;11:1327-35. https://doi.org/10.1016/j.hrthm.2014.04.038
31. Maruyama M, Uetake S, Miyauchi Y, Seino Y,
Shimizu W. Analyses of the Mode of Termination During Diagnostic Ventricular
Pacing to Differentiate the Mechanisms
of Supraventricular Tachycardias. JACC Clin Electrophysiol 2017;3:1252-61. https://doi.org/10.1016/j.jacep.2017.05.014
32. Ito H, Badhwar N, Patel AR, Hoffmayer KS, Moss JD, Pellegrini CN, et
al. Use of Programmed Ventricular Extrastimulus During Supraventricular Tachycardia to
Differentiate Atrioventricular Nodal Re-Entrant Tachycardia From Atrioventricular
Re-Entrant Tachycardia. JACC Clin. Electrophysiol. 2018;4:872-80. https://doi.org/10.1016/j.jacep.2018.01.020
33. Svenson RH, Miller HC, Gallagher JJ, Wallace AG. Electrophysiological evaluation of the Wolff-Parkinson-White syndrome:
problems in assessing
antegrade and retrograde conduction over the accessory pathway.
Circulation 1975;52:552–62. https://doi.org/10.1161/01.CIR.52.4.552
34. Jackman WM, Friday KJ, Fitzgerald DM, Yeung-Lai-Wah JA, Lazzara R. Use of intracardiac
recordings to determine the site of drug action in paroxysmal supraventricular tachycardia. Am J Cardiol 1988;62:8L-19L. https://doi.org/10.1016/0002-9149(88)90010-0
35. Schuger
CD, Steinman RT, Lehmann MH. Recovery of retrograde fast pathway excitability in the atrioventricular node reentrant circuit after concealed
anterograde impulse penetration. J Am Coll Cardiol 1991;17:1129-37. https://doi.org/10.1016/0735-1097(91)90843-X
36. Itagaki
T, Ohnishi Y, Inoue T, Yokoyama M. Linking phenomenon in dual atrioventricular nodal pathways. Jpn Circ J 2001;65:937-40. https://doi.org/10.1253/jcj.65.937
37. Miller JM, Rosenthal ME, Vassallo JA, Josephson ME. Atrioventricular
nodal reentrant tachycardia: studies on upper and lower ‘common pathways’. Circ 1987;75:930-40. https://doi.org/10.1161/01.CIR.75.5.930
38. Hadid
C, Gonzalez S, Almendral J. Atrioventricular nodal reentrant tachycardia: evidence of an upper common
pathway in some patients. Heart Rhythm Case Rep 2018;4:227-31.
https://doi.org/10.1016/j.hrcr.2018.02.004