ORIGINAL ARTICLE
Non-conventional Determinants of Cardiovascular Health
in Latin American Women
Determinantes
no convencionales de la salud cardiovascular de la mujer en Latinoamérica
Alejandra Avalos Oddi1,
Verónica Lía Crosa1, MTSAC, Silvina Verdugo1, María
Romera1, Ivana Patiño1, Yanina
Castillo Costa2, MTSAC, Heraldo D’imperio2, MTSAC,
Bibiana Rubilar1, MTSAC
1 Área
Corazón y Mujer ¨Dra. Liliana Grinfeld” de la
Sociedad Argentina De Cardiología, Buenos Aires, Argentina.
2 Área de
Investigación de la Sociedad Argentina De Cardiología, Buenos Aires, Argentina.
Address for reprints: Alejandra Ávalos Oddi. E-mail: investigación@sac.org.ar
Rev Argent Cardiol 2023;91:252-266. http://dx.doi.org/10.7775/rac.v91.i4.20647
ABSTRACT
Background: Besides traditional risk factors (RF),
non-conventional determinants (NCD) of cardiovascular (CV) health are additional
risk factors in women. Therefore, they should be explored to establish their
prevalence and association with the female gender.
Objective: The aim of this study is to know the prevalence of socioeconomic (SE)
and psychosocial (PS) factors as NCD in CV health in Latin American (LATAM)
women.
Methods: We conducted an observational, cross-sectional study using an
anonymous survey distributed among LATAM women between May and June 2022. The
information gathered included SE and PS NCD, traditional RF and cardiovascular
disease (CVD). Results: A total of 4915 women participated; mean age was 49 ±
13 years. Most respondents (49.6%) lived in Argentina, 55.8% in large cities;
94.4% reported adequate access to healthcare services and 89% had access to some
level of education. Although 79.9% had a paid job, more than half reported
their salary was not commensurate (59.5%) and 26.7% reported exposure to
violence at the workplace. The most prevalent PS factors were low to moderate
level of satisfaction (68.3%), anxiety or irritability (51.9%), apathy,
negative thoughts, or unhappiness (41.7%). Age > 45 years was significantly
associated with overweight, obesity, unemployment, and violence at the
workplace.
On multivariate analysis, sleep disorders (OR 1.7; p =
0.001), living in a city with low population density (OR 0.5; p < 0.001),
violence at the workplace (OR 1.8; p = 0.001), anxiety (OR 1.5; p = 0.001) and
a history of pregnancy complications (OR 1.6; p = 0.022) were independently
associated with CVD.
Conclusion: The prevalence of PS and SE factors affecting the CV
health of LATAM women was significant. Variables such as violence at the
workplace, anxiety, or irritability, living in cities with low population
density, sleep disorders and pregnancy complications were independently
associated with CVD. This survey shows the impact of SE and PS factors as NCD
on the cardiometabolic burden and CV health of women
in LATAM, mainly in those > 45 years.
Key words: Cardiovascular - Diseases - Women - Latin America - Risk Factors -
Psychosocial Factors - Socioeconomic Factors
RESUMEN
Introducción:
Más allá de los factores de riesgo (FR) tradicionales, hay determinantes no
convencionales (DnoC) de la salud cardiovascular (CV)
que operan en las mujeres como factores de riesgo adicional. Es por ello
necesario explorarlos y establecer su prevalencia y vínculo con el género
femenino.
Objetivo:
conocer la prevalencia de los DnoC socioeconómicos
(SE) y psicosociales (PS) y su impacto en la salud CV de la mujer en
Latinoamérica (LATAM).
Material
y métodos: estudio observacional, de corte transversal realizado a través de
una encuesta anónima en mujeres de LATAM entre mayo y junio de 2022. Se
recabaron datos sobre DnoC (SE y PS), FR
convencionales y enfermedad cardiovascular (ECV).
Resultados:
participaron 4915 mujeres con edad media de 49 ±13 años. El 49,6 % residía en
Argentina, el 55,8 % en grandes ciudades, el 94,4 % declaró acceso adecuado a
la salud y el 89 % tuvo acceso a algún nivel de educación. Si bien el 79,9 % expresó
tener trabajo remunerado, más de la mitad refirió percibir un salario no acorde
(59,5 %) y una exposición a la violencia en el ámbito laboral (26,7 %). Los
determinantes PS más prevalentes fueron el bajo a moderado nivel de
satisfacción (68,3 %), la ansiedad o irritabilidad (51,9 %), el desinterés, los
pensamientos negativos o la infelicidad (41,7 %). El grupo de edad mayor de 45
años se asoció significativamente a más sobrepeso, obesidad, desempleo y
violencia laboral.
En
el análisis multivariado se encontró asociación independiente con ECV para el
trastorno del sueño (OR 1,7; p = 0,001), residir en una ciudad de baja densidad
poblacional (OR 0,5; p < 0,001), la violencia laboral (OR 1,8; p = 0,001),
la ansiedad (OR 1,5; p = 0,001) y al haber padecido complicaciones del embarazo
(OR 1,6; p = 0,022).
Conclusión:
se demostró una importante prevalencia de factores PS y SE que impactan en la
salud CV de las mujeres en LATAM. Variables como la violencia laboral, la
ansiedad o la irritabilidad, residir en ciudades de baja densidad poblacional,
así como los trastornos del sueño y complicaciones del embarazo se asociaron de
forma independiente con la ECV. Esta encuesta muestra el impacto de los DnoC SE y PS en la carga cardiometabólica
(CCM) y la salud CV de las mujeres en LATAM, principalmente en aquellas mayores
de 45 años.
Palabras
clave: Enfermedades Cardiovasculares Mujeres
Latinoamérica Factores de Riesgo Factores Psicosociales Factores
Socioeconómicos
Received: 05/15/2023
Accepted: 07/18/2023
INTRODUCTION
The idea that the differences between men and women
are exclusively due to biological differences is a reductionist concept, since
there are emotional and sociocultural differences between both genders. In the
emotional and psychological sphere, women are not only affected by hormonal
fluctuations throughout their lives, but also by the complexity of their
neurocognitive functions, shaped by the culture of different societies
throughout history. (1)
Belonging to certain sociodemographic
groups may have additional adverse health effects; many of these groups are
underrepresented in randomized or observational studies. The factors
contributing to this reality include problems with access to healthcare, low
per capita income, educational level, assignment of multiple tasks and roles,
and gender-based violence. Underrepresentation of women in clinical trials
contributes to the lack of evidence of the impact of cardiovascular disease
(CVD) on them. This could partly explain why CVD continues to
disproportionately affect women, both in those conditions they share with men
and in disorders that are more prevalent in women, as stroke, heart failure
(HF) with preserved left ventricular ejection fraction, and myocardial
infarction (MI) and nonobstructive coronary arteries.
(2)
The Pan American Health Organization (PAHO) states
that 80% of worldwide cardiovascular deaths occur especially in lowand middle-income countries and indicates that the
incidence is the same in men and women. (3)
Poverty and the resulting impact on the psychosocial
sphere have a greater impact on women, who are more likely to suffer a heart
attack than their male counterparts. (4-8) The most marginalized and
poorest populations are at greater risk for CVD, and among these populations,
women are the most prone to suffer such episodes. (4)
In Latin America, unfavorable socioeconomic conditions
have a major impact on female gender, affecting quality of life and access to
decent housing, healthy diet or scheduled physical exercise, together with poor
access to education since childhood, with unsatisfied basic needs. (9)
Nowadays we count with evidence about the impact of
stressful triggers, as acute-chronic stress, anger-hostility complex,
depression, vital exhaustion, anxiety, and gender-based violence at home and at
the workplace. Low sociocultural, economic, and demographic level, and even harmful
environmental exposures, are associated with higher risk of developing physical
and mental diseases. (4,10-19) Other pollutants, as tropospheric ozone, nitrogen
dioxide and volatile organic compounds, play a role in the development of
diseases. More than 90 percent of the world's population lives in areas where
pollution levels exceed World Health Organization guidelines. The effects of
air pollution are associated with large urban centers, manufacturing centers
and areas with heavy traffic. In addition, we must add "indoor" air
pollution that mainly affects the population of low to middleincome
countries who still cook and heat their homes with firewood or coal. (10,11) All these factors have different effects according to
gender, as in coronary syndromes, ischemia without obstructive coronary
arteries (MINOCA/INOCA), takotsubo syndrome, and X
syndrome. The latter are not associated with traditional risk factors, and
adverse psychological and sociodemographic profiles
seem to play a determining role. We now know that these conditions have a less
benign course than was previously thought. (20,21)
In this context, it is necessary to implement a gender
mainstreaming approach in trials, research, and medical practice. The lack of
attention in this regard constitutes a gender bias or gap that has had a
negative impact on the diagnosis and prognosis of a disease considered not
prevalent in women, when in fact it has been disregarded or ignored. (22)
OBJECTIVE
The aim of this study is to know the prevalence of SE
and PS factors as NCD in CV health in a population of Latin American (LATAM)
women.
METHODS
We conducted an observational, cross-sectional study
using an anonymous survey with closed questions developed in REDCap. The participation was voluntary. The survey was
distributed among women >18 years between May and June 2022 through social
networks (WhatsApp, e-mail, Facebook, and others) of
members and district leaders of the Heart and Women Area of the Argentine
Society of Cardiology (SAC) in different geographic regions of Argentina. The
participation of the Council of Cardiovascular Disease in Women of the South
American and Interamerican Society of Cardiology
(SSC-SIAC) made it possible to distribute the survey in different LATAM
countries. The survey is published in the Appendix. The questions dealt with
personal and occupational psychosocial sphere, gender-based violence (23), and conventional risk factors and CVD.
Statistical analysis
The population was divided into two groups: the first
group was made up of women aged 45 years and the second group of those
respondents > 45 years, to explore differences in the main variables in two
different generations. Mean age of onset menopausal transition (WHO), when estrogen levels decline and cardiometabolic
changes begin to occur, was used to define the cut-off point (Figure 1). The association between non-conventional and
traditional factors was also explored.

Fig. 1. Proportion of participant from the different Latin
American countries
Qualitative variables are presented as frequencies and
percentages. Quantitative variables are expressed as mean ± standard deviation
(SD), or median and interquartile range (IQR 25-75), according to their
distribution.
Discrete variables were analyzed using the chi square
test or Fisher's exact test, as applicable. For continuous variables, the t
test or the Mann-Wihtney test were used, as applicable, and in case of 3 groups
or greater, ANOVA or the Kruskall-Wallis test were used, as applicable. A p
value < 0.05 was considered statistically significant.
All the calculations were performed with the software
package R.
Ethical considerations
The survey was approved by the Committee on Ethics of
the Argentine Society of Cardiology. An informed consent was not required due
to the design of the study.
RESULTS
A total of 4915 women responded the survey. Mean age
was 49 ±13 years.
Fourteen women (0.3%) identified themselves as
belonging to the LGTBIQ+ (acronym for lesbian, gay, bisexual, transgender,
intersex and queer; the plus sign represents people with diverse sexual
orientation and gender identity) community.
Most respondents (49.6%) lived in Argentina, followed
by Uruguay (15.5%), Chile (4.3%) and Peru (3.8%), among other countries (Figure 1).
Of those surveyed, 55.8% lived in large cities and
10.5% in towns. Quick and easy healthcare access was reported by 94.4% of respondents,
and mostly in the private sector (83.6%). Lower population density (< 500
000 inhabitants) was associated with higher body mass index (BMI, 26 vs. 25
kg/m2, p = 0.002) and CVD (9% vs. 5%; p = 0.046).
Most survey respondents have access to basic services,
such as public water system (90.2%), electrical grid (97.9%) and sewage system
(82.5%); only 57% had access to pipe gas.
In terms of marital status, most respondents were
married or had a partner (65.3%) or were cohabiting with a partner or children
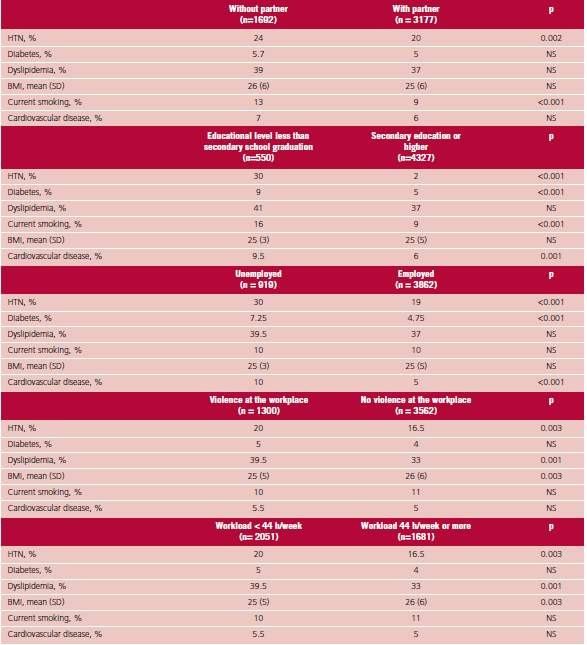
(66.9%). Hypertension (HTN) and tobacco use were more common in those without a
partner (24% vs. 20%, p = 0.002, and 13% vs. 9%, p < 0.001, respectively).
Eighty-nine percent received some level of education
and 4.1% did not complete compulsory education. (24) Educational level less than secondary school
graduation was significantly associated with HTN (30% vs. 2%), diabetes (DM, 9%
vs. 5%) and CVD (10% vs. 5%), in all cases with p < 0.001.
A total of 79.9% had a paid job, half of them were
professionals (51.2%) and most of them were employees (68.7%). Forty-five
percent reported working more than 44 hours per week, mainly those < 45
years (51% vs 40%, p < 0.001); 38.7% considered the workload was excessive
and 85.7% reported their physical and emotional health was compromised. The
variable "salary not commensurate with workload" (59.5%) was
associated with HTN, higher BMI and CVD, in all cases with statistical
significance. Labor inequity in terms of hierarchical positions or remuneration
was reported by 33.8%.
Unemployment was associated with HTN, DM, smoking
habits and CVD (p < 0.001).
Gender-based violence (physical, psychological,
sexual, and institutional violence based on sexual orientation or gender
identity, UN) occurred at the workplace (26.7%) and at home (22.4%). Violence
at the workplace was associated with CVD (8% vs. 5%, p < 0.001), while
violence at home was associated with dyslipidemia (DLP, 40.5% vs. 37%, p =
0.047], higher BMI (26.4 vs. 25.7 kg/m2, p < 0.001) and smoking
habits (15% vs. 9%, p < 0.001, respectively).
A total of 25.4% of the respondents had experienced
sexual violence or sexual abuse during their lifetime, associated with higher
BMI (26.3 vs. 25.7 kg/ m2, p < 0.001) and smoking habits (13% vs.
9%, p < 0.001, respectively).
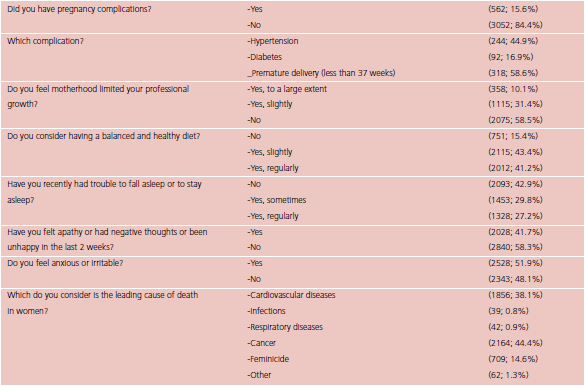
Only 31.7% reported high level of satisfaction in
their personal life. Low to moderate level of satisfaction (68.3%) was
significantly associated with higher cardiometabolic burden, and higher rates
of DBT, DLP, higher BMI, smoking habits, and CVD. Social discrimination was
reported by 19.8%, mainly due to physical appearance; this variable was
associated with higher BMI (p < 0.001), smoking habits (12% vs. 10%, p =
0.043) and CVD (15% vs. 9%, p < 0.001).
Mood disorders (apathy, negative thoughts, or
unhappiness) in the last two weeks (41.7%), were associated with higher rates
of DLP (40% vs. 36%) and smoking habits (13% vs. 9%), while irritability or
anxiety (51.9%) were associated with higher rates of smoking habits, higher
BMI, and CVD (7% vs. 5%, p < 0.001). Sleep disorders (57%) were associated
with DLP (40% vs. 34%) and CVD (7% vs. 4.5%, p < 0.001).
Regarding conventional RF, 21.6% had hypertension and
were taking antihypertensive drugs, 5.2% were diabetics, 10.4% were current smokers
and 30% were former smokers. Tobacco exposure was higher in transgender
respondents (p = 0.026).
More than half of the respondents (54.1%) reported
cholesterol levels > 200 mg/dL, and 48% reported a waist circumference >
or equal to 88 cm.
Forty-six percent had a BMI below 25 kg/m2,
34% had overweight (between 25 and 30 kg/m2), mainly those > 45
years (36% vs. 31%, p < 0.001) and 20% had obesity (BMI > 30 kg/m2),
which was also more common in those > 45 years (22% vs. 17%, p < 0.001). Less
than half (46.4%) of the women surveyed perform at least 150 minutes of
physical exercise per week; 63.9% mentioned having little or no time for
personal leisure activities. A total of 58.8% did not follow a balanced and
healthy diet; 9.5% drank more than 100 g of alcohol per week and 5.3% took
drugs; both variables were associated with a higher prevalence of smoking
habits.
Annual heart health check was reported by 43.4% and
77.5 % underwent an annual gynecological exam. Cardiovascular disease was reported
by 6.6%: arrhythmias (50.3%), coronary artery disease (21.8%),
heart failure (21.5%), cerebrovascular disease (9.7%),
aortic and peripheral artery disease (6.7%) and renal artery disease (0.7%).
Regarding coronary artery disease, 46.8% reported a history of angina, 35.5%
myocardial infarction, 30.6% percutaneous coronary intervention with or without
stenting, and 19.4% myocardial revascularization surgery.
Half of the respondents (50.3%) were taking some type
of medication on a regular basis. The most commonly used drugs were
antihypertensive agents (34.6%), lipid-lowering agents (21.7%) and
anxiolytics/antidepressants (25.2%).
When asked about the obstetric history, 72.8%
responded having at least one pregnancy and 15.6% of them reported one or more
of the following complications: hypertension (44.9%), premature delivery
(58.6%), miscarriage (2.9%), voluntary termination (1.1%) and gestational
diabetes (16.9%). An adverse obstetric history was associated with HTN (32 %
vs. 23 %, p < 0.001), DM (10 % vs. 5 %, p < 0.001), higher BMI (27 vs. 26
kg/m2, p < 0.001) and current CVD (9 % vs. 5 %, p = 0.022).
Cancer was considered the leading cause of death in
women by 44.4% of respondents, followed by CVD (38.1%) and feminicide (14.4%).
On multivariate analysis, sleep disorders (OR 1.7, p =
0.001), living in a city with low population density (OR 0.5, p < 0.001),
violence at the workplace (OR 1.8, p = 0.001), anxiety (OR 1.5, p = 0.001) and
a history of pregnancy complications (OR 1.6, p = 0.022) were independently
associated with CVD.
Age > 45 years was significantly associated with
overweight, obesity, unemployment, and violence at the workplace, while sexual
violence, higher workload with commensurate salary and higher educational level
were related with age < or equal to 45 years (Figure 2).

Fig. 2. Significant factors by age
DISCUSSION
This survey shows the impact of self-referred PS and
SE determinants on the cardiometabolic burden (CMB) and CV health of women in
LATAM, mainly in those > 45 years.
In Latin America, the proportion of overweight and
obese adults has significantly increased in recent decades, (25) and this epidemic has spread to lowand middle-income
countries. Malnutrition in all its forms, whether overweight, obesity or
undernutrition, is associated with poverty. (26) In Argentina, the prevalence of overweight and
obesity over the years has shown a clear upward trend, particularly in the most
socially vulnerable groups. (27)
A multinational South American cohort examined
variations in the incidence and mortality rates of CVD and analyzed the contribution
of modifiable risk factors to the development of CVD and to all-cause death.
Deaths were higher in rural areas compared to urban areas, and low educational
level ranked as the third risk factor. (28) In addition, exposure to an excessive workload
associated with dissatisfaction with the salary earned in relation to workload,
together with inequity, constitute chronic stress factors that affect mental
and physical health (85.7%), a situation that was exacerbated during the
COVID-19 pandemic (the prevalence of depression and anxiety in Argentina
reached 36.4%). (29,30) Mood disorders as apathy, negative thoughts or
unhappiness in the last two weeks, and irritability or anxiety were
significantly associated with higher CMB and CVD.
In 2021, the American Heart Association (AHA)
published a scientific statement associating certain positive psychological
factors (e.g., optimism, sense of purpose, happiness) and negative
psychological factors (e.g., stress, depression, anxiety) to CV health and CV
risk, respectively. (31) Emotional distress is considered a risk factor
associated with increased CMB and CVD with increased platelet reactivity, risk
of coronary heart disease, and incidence of depression, anxiety, and suicide. (32-34)
Gender-based violence is an emerging risk factor that
begins early, affects adolescents and young women, and is more prevalent in
low-income countries over lifetime. (35) In the population surveyed, gender-based violence
occurred both at the workplace (26.7%) and at home (22.4%) representing a
global public health problem and a violation of human rights.
(36) Even cardiometabolic disorders
developed after a childhood marked by abuse can lead to unhealthy lifestyle
habits (sedentary lifestyle, unhealthy diet, sleep disorders, use of toxic
substances and smoking) and psychological disorders (post-traumatic stress)
with an impact on the immune, metabolic, neuroendocrine, and autonomic nervous
systems. (37)
Sleep disorders were associated with CVD in the
surveyed population. During 2022, the AHA published "Life's Essential
8" (LE8). (38) This update document included "quality of
sleep" as an essential factor. The evidence demonstrates that fragmented
sleep and inappropriate sleep duration (short duration, < 6 h, or long
duration, > 9 h) is associated with increased morbidity and mortality, primarily
from cardiovascular disorders and increased risk of type 2 diabetes.
(39) Furthermore, short and fragmented sleep patterns are
independently associated with higher atherosclerotic plaque burden in middle-aged
individuals in multiple territories. (40)
CONCLUSION
We demonstrated a significant prevalence of PS and SE
factors affecting the CV health of women in LATAM, where variables such as
violence at the workplace, anxiety, or irritability, living in cities with low
population density, sleep disorders and pregnancy complications were
independently associated with CVD. This is the most extensive survey to date
showing the impact of SE and PS factors as NCDs on the CMB and CV health of
women in LATAM, mainly in those > 45 years.
In this context, it is necessary to implement a gender
mainstreaming approach in trials, research, and medical practice. The lack of
attention in this regard constitutes a gender bias or gap that has had a
negative impact on the diagnosis and prognosis of CVD in women.
Changes in policies, education and training,
innovations in health care delivery, and diversification of cardiology are
essential to overcome disparities that affect cardiovascular health in LATAM
women. It is necessary to think of women as part of a whole rather than a
simple part of a whole.
Study limitations
As this study is based on a non-probabilistic sample,
it is difficult to accurately establish the prevalence of RFs in the target
population. There is also a disproportion among respondents, with high
participation of Argentine women and low representation of the rest of LATAM
countries. The information gathered was self-reported by the participants,
without corroborating the answers.
Conflicts of interest
None declared.
(See authors’ conflict of interests forms on the web).
Financing
None.
![]() https://creativecommons.org/licenses/by-nc-sa/4.0/
https://creativecommons.org/licenses/by-nc-sa/4.0/
©Revista Argentina de Cardiología
1. Lopez Rossetti D. Ellas. Cerebro,
corazón y psicología de la mujer. 2016 Editorial Planeta. ISBN 978-950-49-5125-4
2. Lindley
KJ, Aggarwal NR, Briller JE, Davis MB, Douglass P, Epps KC, et al. Comité de Enfermedades
Cardiovasculares en mujeres del Colegio Americano de Cardiología y el Grupo de
Trabajo de Equidad en Salud del Colegio Americano de Cardiología. Socioeconomic Determinants of Health and
Cardiovascular Outcomes in Women. JACC 2021;78:1919-29. https://doi.org/10.1016/j.jacc.2021.09.011
3. La salud en las Américas
Organización Panamericana de la Salud, Pan American Health Organization. https://www.paho.org/es
4. Vogel
B, Acevedo M, Appelman Y, Bairey
Merz CN, Chieffo A, Figtree GA, et al. The Lancet women and cardiovascular disease Commission: reducing the
global burden by 2030. Lancet. 2021;397:2385-438. https://doi.org/10.1016/S0140-6736(21)00684-
5. Pan
American Health Organization and WHO. Mortality in the Americas. https://www.paho.org/salud-en-las-americas2017/?tag=cardiovascular-diseases (accessed April 23, 2021).
6. Tejero
ME. Cardiovascular disease in Latin American women. Nutr
Metab Cardiovasc Dis 2010;20:405-11. https://doi.org/10.1016/j.numecd.2010.02.005
7. Xu X,
Bao H, Strait KM, Edmondson DE, Davidson KW, Beltrame JF, et
al. Perceived stress after acute myocardial infarction: a comparison between
young and middle aged women versus men. Psychosom Med 2017;79:50-8. https://doi.org/10.1097/PSY.0000000000000429
8. Anand
SS, Razak F, Davis AD, Jacobs R, Vuksan V, Teo K, et al. Social disadvantage
and cardiovascular disease: development of an index and analysis of age, sex,
and ethnicity effects. Int J Epidemiol 2006;35:1239-45. https://doi.org/10.1093/ije/dyl163
9. www.paho.org/es/temas/determinantes-sociales-salud.
10. Norris
CM, Yip CY, Nerenberg KA, Clavel MA, Pacheco C, Foulds HJ. State of the Science
in Women’s Cardiovascular Disease: A Canadian Perspective on the Influence of
Sex and Gender. J Am Heart Assoc. 2020;9:e015634. https://doi.org/10.1161/JAHA.119.015634
11.
Rajagopalan S, Al-Kindi SG, Brook RD. Air Pollution and Cardiovascular Disease.
JACC State-of-the-Art Review. J Am Coll Cardiol 2018;72:2054-70. https://doi.org/10.1016/j.jacc.2018.07.099
12. Brauer
M, Casadei B, Harrington R, Kovacs R, Sliwa K. Taking a stand against air
pollution – the impact on cardiovascular disease. A joint opinion from the World
Heart Federation, American College of Cardiology, American Heart Association,
and the European Society of Cardiology. Eur Heart J 2021;0:1-4. https://doi.org/10.1161/CIRCULATIONAHA.120.052666
13. World
Health Organization. WHO | Violence Against Women. WHO; 2018. Available at: http://www.who.int/mediacentre/factsheets/fs239/en/
14. Maas
AH, Rosano G, Cifkova R, Chieffo A, van Dijken D, Hamoda H. Cardiovascular
health after menopause transition, pregnancy disorders, and other gynaecologic
conditions: a consensus document from European cardiologists, gynaecologists,
and endocrinologists. Eur Heart J 2021:00:1-18. https://doi.org/10.1093/eurheartj/ehaa1044.
15. Arnett
DK, Blumenthal RS, Albert MA, Buroker AB, Zachary D, Goldberger EH, et al.
ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report
of the American College of Cardiology/American Heart Association Task Force on
Clinical PracticeGuidelines. Circulation. 2019;140:e596–e646. https://doi.org/10.1161/CIR.0000000000000678
16. Piepoli
MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. European
Guidelines on cardiovascular disease prevention in clinical practice: The Sixth
Joint Task Force of the European Society of Cardiology and Other Societies on
Cardiovascular Disease Prevention in Clinical Practice (constituted by
representatives of 10 societies and by invited experts). Eur Heart J
2016;37:2315-81. https://doi.org/10.1093/eurheartj/ehw106
17. Cho L,
Davis M, Elgendy I, Epps K, Lindley KJ, Mehta PK, et al, for the ACC CVD Womens
Committee Members. Summary of Updated Recommendations for Primary Prevention of
Cardiovascular Disease in Women JACC State-of-the-Art Review. JACC 2020;75:2602-18. https://doi.org/10.1016/j.jacc.2020.03.060
18. Agarwala A, Michos ED, Samad Z, Ballantyne CM, Virani SS. The Use of Sex-Specific Factors in the
Assessment of Women’s Cardiovascular Risk. February18, 2020. Circulation.
2020;141:592-9. https://doi.org/10.1161/CIRCULATIONAHA.119.043429
19. Young
L, Cho L. Unique cardiovascular risk in women. Heart 2019;0:15. https://doi.org/10.1136/heartjnl-2018-314268
20. Shimokawa H, Suda A, Takahashi
J, Berry C, Camici PG, Crea F, et al, en nombre del Grupo de Estudio
Internacional de Trastornos Vasomotores Coronarios (COVADIS). Características y
pronóstico clínico en pacientes con angina microvascular: Un estudio de cohorte
internacional y prospectivo por el grupo de estudio internacional de estudio de
trastornos vasomotores. COVADIS. Eur Heart
J 2021;00:1- 9. https://doi.org/10.1093/eurheartj/ehab282
21. Figtree
GA, Vernon ST, Hadziosmanovic N, Sundström J, Alfredsson J, Arnott C, et al.
Mortality in STEMI patients without standard modifiable risk factors: a
sex-disaggregated analysis of SWEDEHEART registry data) The Lancet. https://doi.org/10.1016/S0140-6736(21)00272-5
22. van Diemen J, Verdonk P,
Chieffo A, Regar E, Mauri F, Kunadian V, et al. La importancia de lograr la
equidad basada en el sexo y el género en los ensayos clínicos: un llamado a la
acción. Eur Heart J 2021;42:2990-4. https://doi.org/10.1093/eurheartj/ehab457
23. ONU
Mujeres. Preguntas
frecuentes: Tipos de violencia contra las mujeres y las niñas [Internet]. ONU
Mujeres. Available from: https://www.unwomen.org/es/what-we-do/ending-violence-against-women/faqs/types-of-violence
24. https://www.argentina.gob.ar/sites/default/files/ley-de-educ-nac-58ac89392ea4c.pdf
25.
FAO-OPS-WPF-UNICEF (2018).
26. OPS-OMS
(2014). Monteiro,
Moura, Conde y Popkin (2004). McLaren (2007). Dinsa, Goryakin, Fumagalli y
Suhrcke (2012). Ver informe de la 2° Encuesta Mundial de Salud Escolar,
desarrollada por el Ministerio de Salud y Desarrollo Social de la Nación, en: http://www.msal.gob.ar/ent/images/stories/vigilancia/pdf/2014-09_informe-EMSE-2012.pdf
27. Ver informe de la Tercera
Encuesta Nacional de Factores de Riesgo para Enfermedades No Transmisibles,
desarrollada por el Ministerio de Salud y Desarrollo Social de la Nación, en: http://www.msal.gob.ar/images/stories/bes/graficos/0000000544cnt-2015_09_04_encuesta_nacional_factores_riesgo.pdf.
Ver Programa Nacional de Salud
Escolar. Situación de niños, niñas y adolescentes en Argentina. 2019.
Disponible en: http://www.msal.gob.ar/images/stories/bes/graficos/0000001405cnt-Valoracin-antropomtrica-inicio-y-al-finalizar-ciclo-educacin-primaria-Argentina-07-03-2019.pdf.
Ver Sobrepeso y obesidad en niños,
niñas y adolescentes según datos del primer nivel de atención en la Argentina,
publicado por el Ministerio de Salud y Desarrollo Social en 2018. Disponible
en: http://www.msal.gob.ar/images/stories/bes/graficos/0000001387cnt-2019-01_sobrepeso-y-obesidad.pdf.
28. Lopez-Jaramillo P, Joseph P,
Lopez-Lopez JP, Lanas F, Avezum A, Diaz R, et al. Risk factors, cardiovascular disease, and mortality in South America: a
PURE substudy. Eur Heart J 2022;43:2841-51.
https://doi.org/10.1093/eurheartj/ehac113
29. T.D.
Shanafelt, C.P. Oeste, Sinsky C et al Changes in burnout and satisfaction with
work-life integration in physicians and the general workforce between 2011 and
2017. Mayo Clin Proc. 2019;94:1681-94. https://doi.org/10.1016/j.mayocp.2018.10.023
30.
Santomauro DF, Mantilla Herrera AM, Shadid J, Zheng P, Ashbaugh C, Pigott DM,
et al. Prevalencia
mundial y carga de trastornos depresivos y de ansiedad en 204 países y
territorios en 2020 debido a la pandemia de COVID-19. Lancet 2021;398;1700-12.
31. Levine GN, Cohen BE, Commodore-Mensah
Y, Fleury J, Huffman JC, Khalid U, et al. Psychological
Health, Well-Being, and the Mind-Heart-Body Connection: A Scientific Statement
From the American Heart Association. Circulation. https://www.ahajournals.org/doi/10.1161/CIR.0000000000000947
32. Chandan
JS, Thomas T, Bradbury-Jones C, Taylor J, Bandyopadhyay S, Nirantharakumar K.
Risk of Cardiometabolic Disease and All- Cause Mortality in Female Survivors of
Domestic Abuse. J Am Heart Assoc 2020;9:e014580. https://doi.org/10.1161/JAHA.119.014580.
33.
Goldstein BI, Carnethon MR, Matthews KA, McIntyre RS, Miller GE, Raghuveer G,
et al. Major Depressive Disorder and Bipolar Disorder Predispose Youth to
Accelerated Atherosclerosis and Early Cardiovascular Disease. Circulation.
2015;132:965-86. https://doi.org/10.1161/CIR.0000000000000229
34. UK
Government. Guidance: Domestic Violence and Abuse. UK Gov; 2016. Available at: https://www.gov.uk/government/news/new-definition-of-domestic-violence.
35.
Sardinha L, Maheu-Giroux M, Stöckl H, Meyer SR, García-Moreno C. Global,
regional, and national prevalence estimates of physical or sexual, or both,
intimate partner violence against women in 2018. Lancet 2022;399:803-13.
36. World
Health Organization. WHO | Violence Against Women. WHO; 2018. Available at: 38 http://www.who.int/mediacentre/factsheets/fs239/en/
37. Suglia
SF, Koenen KC, Boynton-Jarrett R, Chan PS, Clark CJ, Danese A, et al. Childhood
and adolescent adversity and cardiometabolic outcomes: a scientific statement
from the American Heart Association. Circulation. 2018;137:e15-28. https://doi.org/10.1161/CIR.0000000000000536
38. “Life’s
Essential 8: Updating and Enhancing the American Heart Association’s Construct
of Cardiovascular Health: A Presidential Advisory From
the American Heart Association”.Circulation. 2022;146:e18-e43. https://doi.org//10.1161/CIR.0000000000001078
39. Tobaldini, E., Fiorelli, E.M.,
Solbiati, M. et al. Corta duración del sueño y riesgo cardiometabólico: desde
la fisiopatología hasta la evidencia clínica. Nat Rev Cardiol 16, 213–224
(2019). https://doi.org/10.1038/s41569-018-0109-6.
40. Domínguez F, Fuster V,
Fernández-Alvira JM, Fernández-Friera L, López-Melgar B, Blanco-Rojo R, et al. Association of Sleep Duration and Quality With
Subclinical Atherosclerosis. J Am Coll Cardiol 2019;73:134-44. https://doi.org/10.1016/j.jacc.2018.10.060
APPENDIX
1) Analysis
of variables


BMI: body mass index; HTN: hypertension; SD: standard
deviation
2) Questionnaire of non-conventional determinants in
Latin American women