
Epicardial adipose tissue (EAT) is a layer of visceral its proximity to the myocardium has pathophysiologifat found between the myocardium and the visceral cal implications. In conditions like obesity, EAT inpericardium. EAT is more than just an energy depot. creases and has been identified as a metabolically acIt has important paracrine and endocrine activity, and tive organ capable of releasing proinflammatory and proatherogenic molecules including tumor necrosis factor-alpha, interleukins 1 and 6, leptin, and angiotensinogen. (1)
Current evidence shows that increased EAT volume or thickness correlates with a higher prevalence of diastolic dysfunction, independent of other factors of general or visceral adiposity. (2) Patients with obesity-related heart failure with preserved ejection fraction (HFpEF) often exhibit significant symptoms, physical limitations, and a high risk of cardiovascular death. (3) In this context, EAT appears to play a relevant pathogenic role, as its expansion and remodeling are associated with increased myocardial stiffness, endothelial dysfunction, and fibrosis, which exacerbate diastolic dysfunction. (4) Diastolic dysfunction, an early and core marker in the pathophysiology of HFpEF, is characterized by impaired ventricular relaxation and filling, usually precedes the development of clinical symptoms of HFpEF, and can be detected before symptomatic heart failure develops. (5) Observational and cohort studies have demonstrated that the presence of diastolic dysfunction, as determined by echocardiographic parameters such as the E/e' ratio, septal and lateral e' wave velocity, left atrial volume, and filling pressure, is associated with an increased future risk of developing HFpEF and related cardiovascular events.
EAT can be measured using two-dimensional echocardiography, a technique that requires minimal operator training (6) and correlates well with measurements obtained by computed tomography (CT) or nuclear magnetic resonance imaging (MRI). The aim of this study was to assess EAT thickness by echocardiography in a group of patients with type 2 diabetes without cardiovascular disease and to examine its association with parameters of diastolic dysfunction as a potential risk marker for the development of HfpEF.
METHODS
The registry of diastolic dysfunction in patients with type 2 diabetes (T2DM) of the Council on Cardiometabolism of the Argentine Society of Cardiology included 229 patients < 65 years without cardiovascular disease and adequate ultrasound window, evaluated on an outpatient basis with transthoracic color Doppler echocardiography and tissue Doppler echocardiography. Patients with clinically established cardiovascular disease, blood pressure >140/90 mmHg during Doppler echocardiography, atrial fibrillation, or kidney disease were excluded from the study. The registry had a pre-specified (but non-mandatory) option to measure EAT. Therefore, EAT was measured in 86 non-correlative patients, with measurements taken at convenience. The protocol specified the methodology for assessing epicardial fat with images and a training video. Images were obtained from standard parasternal long-axis and short-axis 2D views to allow for the most accurate measurement of epicardial fat thickness in the right ventricle with optimal cursor beam orientation in each view. On echocardiography, epicardial fat is generally identified as the relatively echo-free space between the outer wall of the myocardium and the visceral layer of the pericardium. Its thickness was measured perpendicularly on the free wall of the right ventricle at endsystole in three cardiac cycles at the point on the free wall of the right ventricle along the midline of the ultrasound beam perpendicular to the aortic annulus which was used as an anatomic landmark.
Although there is no cutoff point for defining increased EAT, thickness values > 4-5 mm or >7 mm were considered abnormal in different epidemiological studies. (7) In our study, a value > 5 mm was considered increased EAT thickness. Mean values were compared with the different functional or structural abnormalities related to the possibility of diastolic dysfunction according to 6 evaluation criteria recommended by the guidelines of the American Society of Echocardiography and the European Association of Cardiovascular Imaging: left atrium (LA) ≥ 34 mL/m2, E/A ratio <0.8, E/e' ratio >14, septal e' <7 and lateral e' <10, tricuspid regurgitation velocity >2.8 m/s. (8)
Informed consent was obtained prior to inclusion in the protocol. The protocol was submitted to the Computerized Registration Platform for Health Research (PRIISA) of the City of Buenos Aires and was approved by the Research Area of the Argentine Society of Cardiology. The study was conducted following the ethical principles of the Declaration of Helsinki. (9)
All the statistical calculations were performed using Jamovi 2.6.24.0 software package. Statistical methods included univariate descriptive statistics (mean, median, and frequency) and chi-square test, Student's t-test, and correlation and linear regression tests. A two-tailed p-value < 0.05 was considered statistically significant.
RESULTS
Of the 229 patients, EAT was measured in 86, who were included in this analysis. Mean age was 56 ± 8.8 years, 53.2% were women, 62.8% were obese, defined as body mass index (BMI) ≥ 30, mean BMI was 31.2 ± 5.3 kg/m2 and 67.1% had hypertension. Mean systolic blood pressure (SBP) and diastolic blood pressure (DBP) values were 129 ± 11 and 79.5 ± 7.4 mmHg, respectively. Regarding treatment with cardioprotective antidiabetic drugs, 10 patients (11.6%) were taking sodium-glucose cotransporter 2 (SGLT2) inhibitors and 8 patients (9.3%) were on glucagon-like peptide-1 receptor agonists (GLP-1RAs). None of the patients had wall motion abnormalities, left ventricular hypertrophy, or significant valvular heart disease. Table 1 shows the morphological and functional abnormalities evaluated by echocardiography according to the presence of increased EAT thickness Mean EAT was 7.07 mm ± 3.09 mm; 65.1% (n = 56) presented EAT thickness >5 mm and 45.5% (n = 39) had EAT thickness >7 mm.
Table 1
Echocardiographic abnormalities by increased epicardial adipose tissue (EAT) thickness
| n | % | EAT ≤ 5 mm (n=30) | EAT > 5 mm (n=56) | p-value | |
|---|---|---|---|---|---|
| LA ≥34 mL/m 2 | 25 | 29.7 | 3.3% (1) | 42.8% (24) | <0.001 |
| E/A < 0.8 | 56 | 65.1 | 60% (18) | 67.8% (38) | 0.485 |
| E/e'> 14 | 2 | 2.3 | 3.3% (1) | 1.8% (1) | 1 |
| Septal E' < 7 cm/s | 56 | 65.1 | 80% (24) | 57.1% (32) | 0.034 |
| Lateral E' < 10 cm/s | 45 | 52.3 | 50% (15) | 53.6% (30) | 0.822 |
| Tricuspid regurgitation velocity > 2.8 m/s | 2 | 2.3 | 0% (0) | 3.6% (2) | 0.540 |
LA: Left atrium
In patients with EAT > 5 mm, 42.9% had > 2 criteria for diastolic dysfunction, vs. 6.7% of those with EAT ≤ 5 mm (p = 0.001).
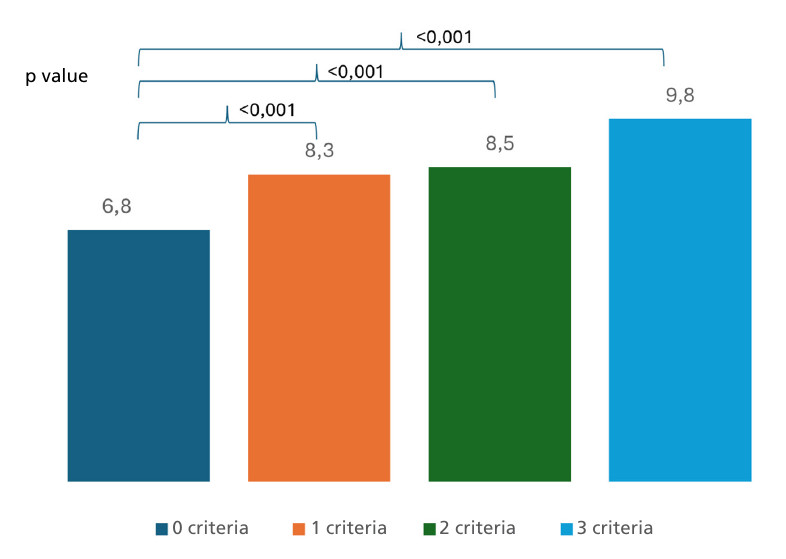
When there were 0 criteria for diastolic dysfunction, mean EAT was 6.8 mm; with 1 criterion, mean EAT was 8.3 mm (p < 0.001 vs. 0 criteria), with 2 criteria mean EAT was 8.5 mm (p < 0.001 vs. 0), and with 3 criteria mean EAT was 9.8 mm (p < 0.001 vs. 0) (Figure 1). There were no patients with a combination of 4, 5, or 6 criteria.
DISCUSSION
In our study, we analyzed a group of patients with T2DM without cardiovascular disease and observed an association between structural and functional abnormalities on echocardiography and increased EAT thickness. Most of our patients with EAT thickness > 5 mm had some form of functional or structural abnormality on echocardiography.
Like any other fat depot, EAT consists of adipocytes, preadipocytes, stromal-vascular cells, nerve cells, and immune cells, with the unique feature of sharing microcirculation and being in close contact with the myocardium. Dysfunctional EAT releases hypoxia-inducible factor-1α (HIF-1α), which increases myocardial nicotinamide adenine dinucleotide phosphate (NADPH) oxidase activity and reactive oxygen species (ROS) production. This promotes hypertrophy through Akt / mammalian target of rapamycin (mTOR) / nuclear factor kappa B (NFkB) pathways, which are related to the development of HFpEF. (10)
EAT tissue assessed by echocardiography has been shown to be an early marker of subclinical cardiac dysfunction, even in obese subjects without overt cardiovascular disease. Interstitial fibrosis, myocardial stiffness, extracellular matrix expansion, and vascular function are key components in the pathogenesis of HFpEF. (11) Increased EAT predicts the onset of diastolic dysfunction before advanced clinical or structural abnormalities become apparent. (12) Cross-sectional studies and meta-analyses have shown that increased EAT thickness or volume correlates with echocardiographic parameters of diastolic dysfunction, such as decreased mitral annular e' velocity and increased E/e' ratio. (13) Furthermore, EAT thickness appears to have prognostic value and could be useful for monitoring therapeutic response in patients with HFpEF and obesity. (14) In patients with severe obesity, an EAT thickness > 5.4 mm measured by echocardiography was independently associated with subclinical cardiac dysfunction. This threshold was identified as a predictor of early functional dysfunction, even in the absence of overt cardiovascular disease. (6) Elevated epicardial fat values, especially > 5-7 mm on echocardiography, should be considered a marker of increased risk for diastolic dysfunction and cardiac functional abnormalities, regardless of other risk factors. (15) In our study, mean EAT thickness was 7.07 mm, with EAT > 5 mm in 65.1% and EAT > 7 mm in 45.5%.
The association between EAT and diastolic dysfunction is particularly relevant in the population of diabetic patients, where it not only functions as a risk marker but may also contribute directly to functional impairment through inflammation, fibrosis, and myocardial stiffness. (16) In our study, patients with EAT >5 mm had a higher prevalence of criteria for diastolic dysfunction. Current clinical evidence demonstrates a correlation between epicardial adiposity and LV diastolic filling or contractility, LV hypertrophy, or atrial remodeling. These findings reflect the clinical manifestation of increased EAT on cardiac metabolism, oxidative stress, inflammation, and fibrosis and, ultimately, the presence of HFpEF. (17) In our study, where the entire population was under 65 years of age and had no established CVD, the presence of significant diastolic dysfunction with three criteria or greater was too rare to draw conclusions in this regard.
Left atrial volume is one of the strongest structural markers for determining diastolic dysfunction. There is a positive and independent relationship between left atrial volume and pericardial fat thickness, and it correlates with greater adverse structural remodeling. (18) In our study, most patients with increased left atrial volume had increased ETT thickness.
CONCLUSIONS
In a group of patients with T2DM without heart disease or significant medical history, the presence of structural or functional abnormalities on echocardiography was associated with increased EAT thickness.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web).