Coronary-Pulmonary
Artery Fistula as Cause of Acute Coronary
Syndrome
Coronary artery fistula (CAF) is a rare congenital or acquired
condition that involves
an abnormal communication between a coronary artery
and either a cardiac chamber
or a great vessel around
the heart. (1) Coronary-pulmonary artery fistulas
account for 15-30% of CAF cases. In general, larger
CAFs present clinical relevance,
focusing mainly on the mechanism of coronary
steal phenomenon, and causing angina and
dyspnea associated to coronary steal and, rarely, to myocardial dysfunction. (3)
We report the case of a 55-year-old woman with a history of arterial hypertension, poor
adherence to treatment, and no
history of surgeries, cardiac events or
trauma. She was admitted to the emergency room
with a 24-hour history of moderate, pulsatile, holocranial
headache, and moderate to severe oppressive retrosternal pain radiating to the shoulder
and left arm, with dyspnea
and generalized pallor.
Physical examination revealed
blood pressure 200/70 mmHg, breathing rate 20 cpm, and arterial oxygen saturation 94%. ECG showed sinus
rhythm, 58 bpm, negative T waves in anteroseptal and
high lateral wall, and absence of Q
waves (Figure
1A). Laboratory data: Troponin T 82 ng/mL,
CK-MB 9.34 ng/mL. Transthoracic
Doppler echocardiography revealed left ventricular ejection fraction (LVEF)
60%, apical hypokinesis, grade I diastolic dysfunction, absence of pericardial effusion or intracavitary
thrombi, and no pulmonary hypertension (PH).

Fig. 1. A. ECG on
admission. Negative T waves in leads DI, aVL, V2- V6 (high lateral
and anteroseptal wall). B. ECG at discharge. Improved
left ventricular repolarization in leads DI,
aVL and V1-V6.
The patient was referred
to the Interventional Cardiology Department with a diagnosis
of non-ST segment
elevation acute myocardial
infarction (AMI). Coronary angiography (CAG) targeted no lesions in epicardial coronary
arteries and a coronary fistula
originating from the distal segment of the right coronary
artery (RCA) and draining into the right pulmonary circulation, a medium-sized vessel with a caliber of 2.5 mm in the proximal portion
(Figure 2 A and B). Left ventriculography showed apical and inferoapical hypokinesis and slightly
decreased contractile reserve.

Fig. 2. A
& B. Angiography of the right coronary
artery (RCA). Dominant artery without
lesions; medium-sized fistula
of distal origin and tortuous trajectory (white arrow)
draining into the pulmonary circulation (white circle). C. Final angiography of the RCA. Closure of the coronary-pulmonary artery fistula, coils (white arrow), and patent RCA in all branches with no evidence
of dissection, thrombus
or embolization.
Percutaneous embolization beyond the first curve of the fistula
using 3 coils (4.0 mm x 7 cm, 5.0 mm x 10
cm and 3 mm x 9 cm) was successfully performed
without complications, confirmed
by the final angiography (Figure 2 C). The patient was discharged asymptomatic and with ECG
improvement on the third day of
hospitalization (Figure 1 B). ECG showed preserved systolic function, normal
pulmonary pressure, and no wall contractility abnormalities.
The first reported case of a coronary artery fistula was in 1865 by Krause; it is mostly a
congenital vascular malformation of relatively low incidence —0.3% of congenital heart disease—, but it is the
most common hemodynamically
significant congenital defect of the coronary
arteries, comprising the 13–14% of the angiographically
recognized coronary artery anomalies. (3, 4) Most CAFs originate from the RCA or anterior descending artery, and drain into
low-pressure structures including right-sided chambers, pulmonary artery, superior vena cava, and coronary
sinus. (4, 5)
CAFs are usually
small, asymptomatic, and are diagnosed
incidentally on imaging
tests. CAFs often
close spontaneously; however,
larger or multiple
CAFs—depending on the degree of severity of the shunt or coronary sequestration— are associated
with symptoms such as fatigue, dyspnea,
palpitations and/or angina. (2, 6) Possible complications include volume overload,
myocardial hypertrophy and congestive heart failure, or myocardial
ischemia/infarction in the absence
of coronary atherosclerosis, arrhythmias, PH,
endocarditis or rupture.
(1, 2)
In our case, we concluded that angina was due to increased myocardial oxygen requirement secondary to high blood pressure. Mechanically, we
considered that anteroapical myocardial ischemia was caused by a steal
effect to the anterior descending
artery circulation through the septal branches, since
the fistula originated from the distal segment of the RCA. Our classification was type-2 AMI due to elevated cardiac
enzymes.
Medium-sized CAFs should be closed in symptomatic
patients, while larger CAFs should be closed regardless of symptoms. (5, 6) Therapeutic strategies depend on the anatomy of the fistula,
its clinical presentation and the team's experience, and a surgical or percutaneous technique can be chosen, considering the risk and feasibility of the procedure. (2, 5) Despite the
recommendation of surgical ligation over coil embolization, (2) following an individualized approach was beneficial.
In conclusion, CAF is the most common congenital
anomaly of hemodynamically significant coronary arteries.
We recommend treating
all medium-sized CAFs. Over the years, this entity may lead
to further growth of the artery,
resulting in further concomitant cardiac disorders
and therapeutic complexity.
Carlos I.
Soledispa1, Marco Larrea1, Stephanie S. Alberca1,
Ariel Zelaya1, Klinton Sanango1
1 Clínica Sur Hospital,
Department of Interventional Cardiology (Guayaquil, Ecuador).
Carlos I. Soledispa – ISAC/ Clínica
Sur Hospital, Department of Interventional Cardiology (Guayaquil, Ecuador).
Av. Febres Cordero Rivadeneyra y Alfredo Adum - 091910,
Guayaquil, Ecuador.
Address for reprints:
E-mail: carisosu@gmail.com
Conflicts of interest
None declared.
(See authors'
conflict of interests forms on the web/Additional material.)
Ethical considerations
Not applicable.
REFERENCES
1. Urmeneta Ulloa J, Molina Borao I, Ochoa Rea ME, Sánchez-Insa E. Percutaneous closure
of coronary artery
fistula before lung transplantation. Arch Bronconeumol 2017;53:520–1. https://doi.org/10.1016/j.arbres.2017.02.013
2. Sulemankhil I, Mohamed
AH, Gilani SA. Coronary-Pulmonary Artery Fistula Repair With Coil Embolization: A Single Center
Experience. Cureus.2022;14:e28407. https://doi.org/10.7759/cureus.28407
3.
Buccheri D, Dendramis G, Piraino D, Chirco PR, Carità P, Paleologo C, et
al. Coronary artery fistulas as a cause of angina: How to manage
these patients? Cardiovascular Revascularization
Medicine [Internet]. 2015;16:306–9. https://doi.org/10.1016/j.carrev.2015.04.011
4.
Gowda RM, Vasavada BC, Khan IA. Coronary artery
fistulas: Clinical and therapeutic considerations. Int J Cardiol 2006;107:7–10. https://doi.org/10.1016/j.ijcard.2005.01.067
5.
Al-Hijji M, el Sabbagh A,
el Hajj S, AlKhouli M, el Sabawi B, Cabalka A, et al. Coronary Artery Fistulas: Indications, Techniques, Outcomes,
and Complications of Transcatheter Fistula Closure.
JACC Cardiovasc Interv [Internet]. 2021;14:1393-406. https://doi.org/10.1016/j.jcin.2021.02.044
6. Buccheri D, Chirco PR, Geraci S, Caramanno G, Cortese B. Coronary Artery Fistulae:
Anatomy, Diagnosis and Management Strategies. Heart Lung Circ
2018;27:940–51. https://doi.org/10.1016/j.hlc.2017.07.014
http://dx.doi.org/10.7775/rac.v91.i2.20623
Inflammatory Spondyloarthropathy Presenting
as a Sole Manifestation of Left Atrial Myxoma
Cardiac tumors are rare, with an incidence of 0.002%. They may originate from the pericardium or
myocardium, and are primary or secondary, the latter being 20 times more common. (1)
Primary cardiac neoplasms
are infrequent, representing 0.25%. Most of them (75%) are
benign and include myxomas, rhabdomyomas, fibromas,
and lipomas. (2)
Cardiac myxomas represent the
most common benign cardiac tumor. They are found in the left atrium (75%), right atrium (20%), or ventricles
(5%). Clinically, myxomas may occur in asymptomatic
individuals and are detected incidentally, or may cause symptoms usually
related to its mobility, size, and location within the heart. In general, the symptomatic triad
includes systemic (fever, weight loss, fatigue) or cardiac symptoms
(arrhythmias, mitral or tricuspid regurgitation due to interference with valve coaptation, pericarditis,
dyspnea, syncope), and pulmonary and/ or
systemic embolic phenomena. (2) While these are the most common manifestations, unusual forms of presentation have also been described.
Doppler echocardiography is the method of choice to diagnose and determine its
characteristics and hemodynamic impact.
The clinical case of a left atrial myxoma
with an unusual presentation is described below.
We report the case of a dyslipidemic,
ex-smoker 61-year-old woman with no cardiovascular history,
consulting for a several-month history
of sacroiliac arthralgia; laboratory tests revealed
elevated erythrocyte
sedimentation rate (84 mm/h) and C-reactive protein (6.2 mg/L), and no other abnormalities.
After evaluation by the Rheumatology Department, diagnosis was inflammatory spondyloarthropathy
with persistently elevated inflammatory markers not meeting the criteria for rheumatic disease; the positron
emission tomography (PET) scan revealed a single tumor in the left atrium (Figure 1).

Fig. 1. PET showing
hypodense left atrial
mass with moderate
metabolic activity.
Doppler echocardiography showed a rounded, heterogeneous,
sessile left atrial mass attached to the interatrial septum,
with wide anarchic
movement, and in non-invasive contact with the right
upper pulmonary vein. This mass did not interfere with the opening and closing of the mitral valve (Figure 2).
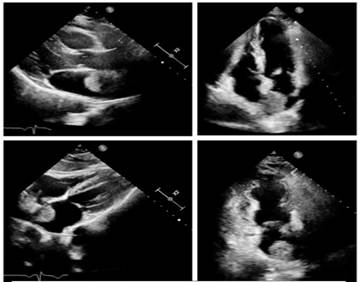
Fig. 2. Doppler echocardiography views showing a rounded, heterogeneous,
left atrial mass attached to the interatrial septum.
CT scan revealed a 30 x 22 mm heterogeneous left atrial mass attached
to the interatrial septum, with regular
borders, enhanced after intravenous contrast
injection, and no evidence of invasion of the pulmonary veins. The
result was interpreted as a possible atrial
myxoma, and surgical resection was performed using a transseptal
approach; a 5 cm tumor was resected without complications, and a biopsy
was sent to Pathology.
Results revealed proliferation of perivascular spindle
cells without atypia, in streaks and in a lax stroma, with
signs of old and recent hemorrhage, scant fibrous tissue and myocytes, consistent with myxoma.
After surgical resection, follow-up showed improvement of joint symptoms until their
disappearance and normalization of inflammatory markers.
Myxomas are the most common benign cardiac tumors, usually found
in older women, (2) as was the case described
here.
They are most commonly found in the left atrium (75%),
as a sessile or pedunculated intracavitary mass, attached by a stalk to the interatrial septum.
Clinical manifestations are related to their cardiac location, size, and mobility. The most
common symptomatic triad includes intracardiac
obstruction, embolism, and systemic symptoms.
According to a French series of 112 cases, heart failure
secondary to mitral valve obstruction was present in 67% of
the patients, followed by cerebral emboli
in 29%, and 34% with general symptoms such as
fever, weight loss or symptoms resembling connective tissue disease. (3)
Intracardiac obstruction often occurs in pedunculated left atrial myxoma protruding to the left ventricle
and causing mitral valve coaptation deficit and subsequent regurgitation. While uncommon,
myxomas found in the right atrium may protrude
into the tricuspid valve and cause
regurgitation. In both cases, they can occur with heart failure
or syncope. (3)
Emboli are more common in papillary myxomas, as they are less solid and
become more fragile with anarchic movement. The site of the emboli
depends on the location of the tumor. Left
atrial myxomas have
the potential for embolism to the central nervous system, resulting in stroke or amaurosis. The involvement of coronary, renal or lower
limb arteries is uncommon.
(4)
Constitutional symptoms may appear as connective tissue disorders, with poor general condition, weight loss, anorexia, and fever. These symptoms are more common in women than in men, and in right atrial myxomas. (4)
It is believed that extracardiac
manifestations are often caused by
embolic phenomena and inflammation due to the intrinsic
secretion of cytokines. (5) Polymyalgia rheumatica —the manifestation that motivated our
patient's consultation— is uncommon. Polymyalgia rheumatica is characterized by pain
in the proximal muscles and
increased serum levels of inflammatory
markers. It is also one of the most common diseases in young adults and affects
women more frequently than men (ratio 3:1). (6)
Doppler echocardiography is essential for the diagnosis of
myxomas, and to define location, size, and complications. Both cardiac magnetic
resonance imaging and cardiac multislice computed
tomography provide additional information for decision making.
Myxoma needs surgical excision
to reduce the risk of embolization. While the rate of recurrence is low, follow-up Doppler echocardiography is recommended. (4) In the case reported, our patient debuted
with rheumatologic manifestations with persistently elevated
inflammatory markers; left atrial myxoma was incidentally found after several diagnostic tests.
Undoubtedly, myxoma remains a
challenging entity to diagnose. The fact that they are typically asymptomatic
or present with nonspecific symptoms makes it a non-suspected entity,
mostly diagnosed incidentally. It is vital to be aware of
the possible cardiovascular and
systemic manifestations to suspect, diagnose and treat myxomas in a timely manner.
Esperanza Raimundo, Roberto Freue, Fernando PiccininiMTSAC, Florencia Castro, Martín Vivas,
Pablo ElissamburuMTSAC
Conflicts of interest
None declared.
(See authors’
conflicts of interest forms on the website/ Supplementary material).
Sources
of funding: None.
Ethical considerations
Not applicable.
REFERENCES
1.
El Sabbagh A, Al-Hijji MA, Thaden JJ,
Pislaru SV, Pislaru C, Pellikka PA, et al. Cardiac Myxoma: The Great Mimicker. JACC Cardiovasc Imaging. 2017;10:203-6.
https://doi.org/10.1016/j.jcmg.2016.06.018
2. Tyebally S, Chen D, Bhattacharyya S, Mughrabi
A, Hussain Z, Manisty C, et al. Cardiac Tumors: JACC CardioOncology
State-of- the-Art Review. JACC CardioOncol. 2020;2:293-311. https://doi.org/10.1016/j.jaccao.2020.05.009
3. Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine (Baltimore). 2001;80:159-72. https://doi.org/10.1097/00005792-200105000-00002
4. Islam AKMM. Cardiac myxomas: A narrative review. World J Cardiol. 2022;14:206-19. https://doi.org/10.4330/wjc.v14.i4.206
5.
Macias E, Nieman E, Yomogida K, Petrucci O, Javidan C, Baszis K, et al. Rare presentation of an atrial myxoma in an adolescent patient: a case report and literature review. BMC Pediatr. 2018;18:373. https://doi.org/10.1186/s12887-018-1313-6
6.
Mano Y, Yoshizawa A, Itabashi Y, Ohki T, Takahashi T, Mori M, et al. Left atrial myxoma detected
after an initial
diagnosis of polymyalgia rheumatica. Intern Med 2014;53:441-4.
https://doi.org/10.2169/internalmedicine.53.1300
http://dx.doi.org/10.7775/rac.v91.i1.XXXXX
Endovascular Treatment of Pulmonary Vein Stenosis After Atrial
Fibrillation Catheter Ablation
Radiofrequency catheter ablation
with pulmonary vein isolation for treatment of atrial fibrillation (AF) is a minimally invasive
procedure with low rate of complications. One complication is pulmonary vein stenosis, with an incidence
between 0.3 and 3.4%, but associated with high morbidity. (1-3) Symptoms of pulmonary
vein stenosis include
dyspnea, cough, hemoptysis, and chest pain. (4) We report a case of hemoptysis
secondary to pulmonary vein stenosis after radiofrequency
catheter ablation, treated with angioplasty and stent implantation.
A 42-year-old male patient with a history of radiofrequency
catheter ablation of the pulmonary veins, performed in another center,
and community-acquired pneumonia which was hard to treat despite
the use of different antibiotic regimes, presented to the emergency
department of our institution 5 months after
the procedure with intermittent hemoptysis and pain in the left hemithorax.
On admission, the patient was hemodynamically stable,
without fever and with no signs of heart failure. The laboratory tests showed: hematocrit 37%; white blood
cell count 5490/mm3, 229 300 platelets/mm3,
erythrocyte sedimentation rate 25 mm/h, and high-sensitivity C-reactive protein level 10.6 mg/L. As acute pulmonary embolism (PE) was
suspected, the patient underwent
chest computed angiotomography, which was negative for PE but showed areas
of ground-glass opacification,
with a tendency to consolidation, that were diffusely distributed in the left
lung upper lobe.
The patient was clinically stable and was discharged
with empiric treatment for suspected atypical pneumonia and was followed up in
an outpatient basis. Because of the
recent history of AF ablation and the
pattern evidenced in the chest computed tomography, we decided to perform
cardiac computed angiotomography to evaluate the
pulmonary veins which had not been
correctly visualized in the angiography requested to rule out PE. The scan showed
stenosis of the left superior
pulmonary vein (LSPV),
with a diameter of 8.4 mm × 17 mm in length,
pronounced narrowing in flute beak
appearance, and critical luminal reduction with a trajectory of about 16 mm
until reaching the patent intraparenchymal portion (Figure 1A). The other pulmonary veins were patent with no signs of stenosis.
In the presence of a patient with hemoptysis and symptoms
of persistent pneumonia
and stenosis of the LSPV, we decided to perform
angioplasty of the pulmonary vein with stent implantation. A transesophageal echocardiogram (TEE) was performed
before the procedure, which demonstrated increased velocities (peak velocity 2.4 m/s, peak gradient 23 mm Hg) in the vein, confirming the diagnosis
(Figure
1B). Transseptal
puncture was carried out through a right femoral
venous access and under TEE guidance. A selective venography confirmed LSPV
stenosis (Figure 2A). Then, coronary balloon catheters with increasing
diameters were advanced for pre-dilation. A conventional stent with high radial strength
(Herculink 7.0 × 18
mm) was implanted, with adequate angiographic results (Figure 2B). Pressures
and velocities decreased in TEE (peak
velocity 1.3 m/s, maximum gradient 7 mm Hg).

Fig. 1. A. Computed angiotomography showing stenosis
of the left superior pulmonary vein (arrow). B. Left superior
pulmonary vein velocity measured by transesophageal echocardiography.
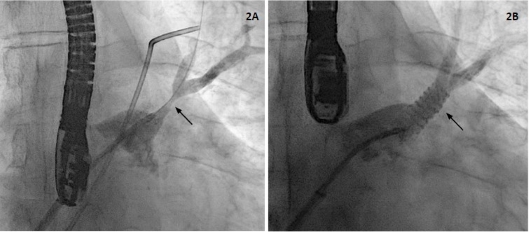
Fig. 2. A. Venography demonstrating stenosis
of the left supe rior
pulmonary vein (arrow). B. Venography
after stent implantation (arrow)
in the left superior pulmonary vein.
The patient was discharged 24 hours later, on anticoagulation with rivaroxaban
15 mg/d and antiplatelet therapy with clopidogrel 75 mg/d.
At 3-month follow-up, dyspnea, cough and pain in
the left side of the chest has disappeared.
Pulmonary vein stenosis
after radiofrequency catheter ablation is a rare and
underdiagnosed complication because symptoms
can be mistaken for other conditions as pneumonia, asthma, and PE, among others. (4) The proper diagnosis of this condition is of utmost importance, as delayed diagnosis can lead
to total occlusion of the pulmonary vein, resulting in pulmonary infarction and massive hemoptysis. Magnetic angioresonance and computed angiotomography
are the most accurate diagnostic
methods for detecting pulmonary vein stenosis. The severity of stenosis is defined by the percentage of lumen involved and is
classified as mild (<50%), moderate (50%-70%) and severe (>70%). The development
of symptoms is usually associated with severe
stenosis or total occlusions, which can sometimes be asymptomatic. Transesophageal echocardiography is a very useful
diagnostic method to guide the procedure,
since it provides information on the structure of the left atrium, optimizes
manipulation of materials as guide wires and balloon catheters during the procedure, and adds the evaluation of pulmonary veins
flow and gradients for the diagnosis
of stenosis and for evaluating treatment effectiveness. (5) In this case, we used
the same procedure to provide diagnosis, guide
transseptal puncture (which is ideally
inferior and anterior for better orientation to the LSPV), measure velocities after
the procedure, and rule out complications as pericardial effusion.
Treatment with angioplasty is intended to relieve venous
pressure and improve
perfusion of the affected lung.
Compared to balloon
angioplasty, stenting is associated
with a lower rate of restenosis, especially when
large stents (10 mm or more) are used. (5,6) Stent size is defined before the procedure by computed angiotomography and during the procedure by angiography,
since the use of stents larger than the vein
could lead to rupture and cardiac tamponade.
Other treatments include lobectomy in
patients with clinically significant pulmonary vein occlusion or stenosis in whom angioplasty has failed. (5)
We report this case of hemoptysis, dyspnea and pain secondary to pulmonary vein stenosis
that was successfully treated
with angioplasty and stent implantation. The recognition of this condition,
its timely diagnosis and adequate treatment is of utmost importance to reduce patient
morbidity.
Conflicts of interest
None declared.
(See authors’
conflicts of interest
forms on the website/ Supplementary material).
Ethical considerations
Not applicable.
Juan I. Damonte1,
Ezequiel Lillo2, Mariano Falconi2, Santiago Sanchez Bustamante2, Carla Agatiello,
Ignacio M. Seropian1
1 Department of Interventional Cardiology, Institute of Cardiovascular Medicine, Hospital Italiano de Buenos Aires, Argentina
2 Department of Cardiology, Institute of
Cardiovascular Medicine, Hospital Italiano de Buenos Aires, Argentina
Address for reprints:
Dr. Ignacio M. Seropian, ignacio.seropian@hospitalitaliano.org.ar
REFERENCES
1. Correction to: Severe Pulmonary
Vein Stenosis Resulting
From Ablation for Atrial Fibrillation: Presentation, Management, and Clinical Outcomes.
Circulation 2017;135(18):e1016. https://doi.org/10.1161/CIR.0000000000000494
2. Cappato R, Calkins H, Chen S-A, et al. Updated
worldwide survey on the methods,
efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol 2010;3:32-8. https://doi.org/10.1161/CIRCEP.109.859116
3. Saad EB, Rossillo A, Saad CP,
et
al.
Pulmonary vein stenosis after radiofrequency ablation
of atrial fibrillation: functional characterization, evolution,
and influence of
the ablation strategy. Circulation 2003;108:3102-7. https://doi.org/10.1161/01.CIR.0000104569.96907.7F
4. Fender EA, Widmer RJ, Hodge DO, Packer DL, Holmes DR Jr. Assessment and Management of Pulmonary
Vein Occlusion After
Atrial Fibrillation Ablation.
JACC Cardiovasc Interv 2018;11:1633- 9. https://doi.org/10.1016/j.jcin.2018.05.020
5. Calkins H, Brugada J, Packer DL, et al. HRS/EHRA/ECAS expert consensus statement on catheter and
surgical ablation of atrial fibrillation: recommendations for personnel,
policy, procedures and follow-up. A report of the Heart Rhythm Society
(HRS) Task Force on
Catheter and Surgical Ablation of Atrial Fibrillation developed in partnership with the European Heart Rhythm
Association (EHRA) and the European
Cardiac Arrhythmia Society (ECAS); in collaboration with the American College
of Cardiology (ACC), American Heart Association
(AHA), and the Society of Thoracic Surgeons (STS). Endorsed and approved by the
governing bodies of the American College of Cardiology, the American Heart
Association, the European Cardiac Arrhythmia
Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons,
and the Heart Rhythm Society. Europace
2007;9(6):335–79. https://doi.org/10.1093/europace/eum120
6. Xuan Z, Liu B, Ci M, Wang Z, Fan Y. Hemoptysis secondary to pulmonary vein stenosis after
radiofrequency ablation for atrial fibrillation: A case report and literature review. J Interv Med 2020;3:98- 100. https://doi.org/10.1016/j.jimed.2020.03.008
http://dx.doi.org/10.7775/rac.v91.i2.20622
Transseptal
Balloon Atrial Septostomy in Patients with Advanced Pulmonary Arterial
Hypertension and Systemic
Lupus Erythematosus
We report the case of a 20-year-old female patient with a diagnosis
of mixed connective tissue disease in 2018 but no follow-up for the last 18
months, and with Hashimoto's
thyroiditis and bronchiectasis. The patient
went to the Outpatient Emergency Room for abdominal
pain, nausea and diarrhea. Signs of right heart
failure (edema of the lower limbs, jugular venous distention without
inspiratory collapse, positive hepatojugular reflux and enlarged liver),
increased intensity of the
second heart sound at the expense of the
pulmonic component, and systolic murmur in the
tricuspid focus were detected on admission. Initial diagnostic tests
included an ECG showing signs of overload of the right chambers and complete
right bundle branch block, and a
chest X-ray with enlarged second right
pulmonary arch and normal cardiothoracic ratio. Doppler echocardiography
revealed enlargement of the right
chambers, severe right ventricular dysfunction, severe tricuspid regurgitation with peak regurgitation velocity > 4.5
meters per second (m/s), pulmonary
artery systolic pressure (PSP) 105 mmHg, mean
pulmonary artery pressure (mPAP) 55 mm Hg, and mild pericardial effusion (Figure 1).

Fig. 1. Doppler echocardiography. Apical
4-chamber view showing marked
enlargement of the right chambers,
displacement of the ventricular septum, reduction
in left ventricular diameter, and severe tricuspid
regurgitation.
Right heart catheterization
confirmed the diagnosis of severe pulmonary arterial hypertension (PAH) with
mean right atrial pressure
11 mmHg, mPAP 63 mmHg, pulmonary
wedge pressure 10 mmHg, pulmonary vascular resistance (PVR)
21 Wood units (WU), transpulmonary and diastolic
gradients of 53 mmHg and 43 mmHg
respectively, cardiac output (CO) 3.20 L/min,
cardiac index (CI) 2.6 L/min/m2, systolic
volume index (SVI) 23 ml/beats/m2, mixed
venous saturation 65%, and arterial
saturation 97%. Due to marked right ventricular failure, the patient was
started on continuous intravenous
infusion of furosemide with no positive response,
inotropic support with high-dose milrinone that was later switched to levosimendan 0.1 ug/kg/ min, and vasopressor support with intermediate doses of
noradrenaline. The patient progressed unfavorably, with low cardiac output and severe right ventricular failure.
Given that immediate
access to parenteral prostanoids was not possible,
transseptal
balloon septostomy
was performed (5 mm fenestration) successfully
(Figure 2). The patient's
clinical condition improved, with early referral to a
tertiary care center for pre-transplant evaluation and continuous intravenous epoprostenol infusion —increasing doses up to 12 ng/kg/min— after weaning and discontinuation of inotropic drugs, and administration
of ambrisentan 10 mg and tadalafil
10 mg, which were well tolerated. Follow-up Doppler echocardiography showed moderate
enlargement of the right chambers, PSP
70 mmHg, and 0.9 mm loss of atrial septal
continuity (Figure 3). Cardiac catheterization showed decreased mPAP and PVR and improved CO and CI (43 mmHg, 7.3 UW, 4.8 l/min and 3.6 l/min/m2,
respectively). After evaluation, the Rheumatology Department confirmed the diagnosis of systemic lupus erythematosus by clinical and immunological criteria, and class II lupus nephritis by renal biopsy.

Fig.
2. Transseptal
balloon septostomy. Balloon dilatation is performed reaching a maximum diameter of 5
mm under fluoroscopic guidance. A: Balloon inflation on guide wire centered
in the atrial septum. B: Total
balloon inflation.

Fig.
3. Long axis parasternal view showing progressive improvement of the right ventricular diameter, reduction of compression to the left ventricle
and ventricular septal hypertrophy.
The prevalence of PAH in connective tissue disease (CTD) is high, mainly in scleroderma and
also in systemic lupus erythematosus, with a value ranging from 0.5 to 17.5%, depending on the diagnostic method used. (1) This entity continues to present high morbidity and mortality
despite the evidence
observed with specific drug
therapies, which is high compared to idiopathic PAH (1-year survival in CTE-PAH 86% vs
93% in idiopathic PAH). (2) Patients not responding
to maximal combination therapy, including parenteral prostanoids,
should be referred for double lung transplant. (3) However, many patients with PAH are not candidates
for transplantation, or the waiting list time is too long and patients die before being transplanted. For this reason, transseptal septostomy should be considered in patients who are
on the waiting list for double lung transplant, in those who do not respond to the maximum therapeutic
regimen or when it is unavailable or not tolerated. (4) It should be noted that this procedure is
contraindicated in patients with arterial
oxygen saturation < 90%, right atrial pressure
> 20 mmHg and hemoglobin value
< 12 mg/dL, and should be performed in referral centers.
Several studies have reported improvement in symptoms and hemodynamics
after septostomy, allowing decompression of the right heart with increased left ventricular pre-load and systemic oxygen
saturation without complications
associated with the procedure in highly experienced centers.
(5)
Recently, a meta-analysis of 6 studies with 204 patients observed
a reduction in right atrial pressure (p< 0.001), an increase in
cardiac index (p < 0.001) and left
atrial pressure (p < 0.001), but with significant reduction in oxygen saturation and 48-hour, and 30- day mortality rates of 4.8% and 14.6%,
respectively. (6)
These data suggest
that atrial septostomy is an invasive and relatively safe procedure in
experienced centers and should only
be indicated in patients with advanced
severe PAH as a bridge to transplantation or
when there is no response to the triple regimen with parenteral prostanoids,
or when drug therapy is unavailable.
Guillermina SorasioMTSAC, 1, Carola ZambranoMTSAC, 1, Susana Taboada1,
Fernando Di Tomasso1, Aldo Peruso5, Enrique Domine1,
Ignacio BluroMTSAC, 2
1 Pulmonary Hypertension Unit,
2 Coronary Care Unit,
3 Department of Doppler Echocardiography,
4 Electrophysiology Service,
5 Department of Interventional Cardiology,
6 Chief of Cardiology.
7 Pulmonary Hypertension, Hospital Italiano. Department of Cardiology - Hospital Rivadavia. Buenos Aires. Argentina. Hospital Italiano de Buenos Aires.
Address for reprints:
guillerminasorasio@gmail.com
Ethical considerations
Not applicable.
Conflicts of interest
None declared.
(See authors’
conflicts of interest forms on the website/ Supplementary material).
REFERENCES
1. Tselios K, Gladman D, Urowitz M.
Systemic lupus erythematosus and pulmonary arterial
hypertension: links, risks, and management strategies. Open Access Rheumatol 2017:9:1-9 https://doi.org/10.2147/OARRR.S123549
2. Chung L, Liu J, Parsons L, Hassoun P, McGoon M, Badesch D, et al. Characterization of connective tissue disease-associated
pulmonary arterial hypertension from REVEAL: identifying
systemic sclerosis as a
unique phenotype. Chest.2010;138:1383-94. https://doi.org/10.1378/chest.10-0260
3. Stacel T, Latos M, Urlik M, Necki M, Antonczyk R, Hrapkowicz T, et al. Interventional and Surgical Treatments for Pulmonary Arteri al Hypertension. J. Clin. Med 2021;10:3326. https://doi.org/10.3390/jcm10153326
4.
Velázquez I, Albarrán A, Jiménez C, García J,
Martín R y Escribano P. Septostomía auricular en el tratamiento de la hipertensión arterial
pulmonar grave del adulto. Rev Esp Cardiol 2016;69:78-81. https://doi:10.1016/j.recesp.2015.09.011
5. Chiu JS, Zuckerman WA, Turner
ME, Richmond ME, Kerstein D, Krishnan U, et al. Balloon atrial septostomy in pulmonary arterial hypertension: effect on
survival and associated outcomes. J Heart Lung Transplant. 2015;34:376-80. https://doi.org/10.1016/j.healun.2015.01.004
6. Khan M, Memon M, Amin E, Yamani N, Khan S, Vincent
M, et al. Use of Balloon
Atrial Septostomy in Patients with Advanced Pulmonary
Arterial Hypertension. A Systematic Review and Meta-Analysis. Chest 2019;156:53-63. https://doi.org/10.1016/j.ijcard.2019.02.051
http://dx.doi.org/10.7775/rac.v91.i2.20617
Portopulmonary
Syndrome Following Liver Transplantation: A Rare Etiology
of Dyspnea that Should Not Be Ignored
We report the case of a 54-year-old male patient with a history of liver transplantation in 2019
due to alcoholic cirrhosis. A right heart catheterization was performed as part of the pretransplant evaluation, due to moderate
pulmonary hypertension (PH) on echocardiography, confirming that PH was
associated with high pulmonary blood
flow and low pulmonary resistances.
Three months after transplantation, the patient came to our emergency room for progressive dyspnea and signs of
pulmonary and peripheral congestion, but stable with nasal cannula oxygen therapy. ECG showed new-onset right bundle branch block. Laboratory
tests revealed elevated D-dimer (2980 ug/mL) and NT-proBNP (10 500 ng/L) levels. A computed angiotomography
of the pulmonary arteries was performed to rule out the initial suspicion of
pulmonary thromboembolism (Figure 1), targeting no thrombi, but revealing marked pulmonary artery
dilation, suggestive of significant PH. Given the poor response to diuretics, the patient was evaluated by
the Cardiology Department at our center.
Transthoracic echocardiography (TTE) (Figure 2) showed marked right ventricular (RV) enlargement and dysfunction, with an estimated pulmonary artery systolic
pressure (PASP) of 120 mmHg, suggestive of severe PH.

Fig. 1. Computed angiotomography
of the pulmonary arteries. Axial planes at the level of ventricular cardiac chambers
and at the level of the great vessels outflow tracts
and bifurcation of the pulmonary
artery (B). No intravascular filling defects in the pulmonary artery or images suggestive of thrombus (B) are observed. RV enlargement is of note, with a right / left ventricle ratio >1 (A). RV: right ventricle.
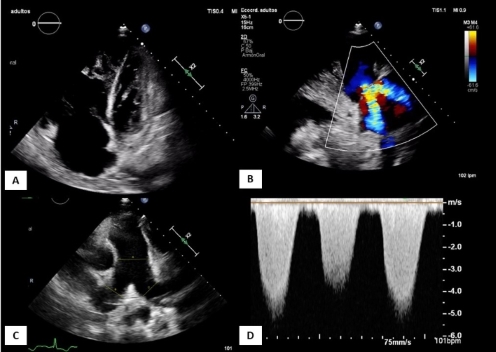
Fig. 2. Transthoracic echocardiography on
admission. Apical 4-chamber
planes (A) modified parasternal long
axis over RV (B), parasternal short axis at the level of great vessels (C) and continuous
Doppler over tricuspid regurgitation flow (D).
Figure (A) shows severe RV
enlargement and dysfunction, with severe
functional tricuspid regurgitation (B).
Enlargement of the
pulmonary artery. The RV-RA gradient of tricuspid regurgitation by Doppler is 120 mmHg (D),
suggestive of severe
PH. PH: pulmonary
hypertension. RA: right atrium. RV: right ventricle
Due to rapid clinical worsening —mainly breathlessness— with increased tachypnea
and signs of heart failure, the patient was referred to the
Coronary Care Unit to start
intravenous therapy with higher doses of dobutamine and furosemide (1 g in continuous infusion).
Evacuative paracentesis for symptomatic management of
ascites was performed, and Doppler ultrasound confirmed proper functioning of
the liver graft. Differential
diagnosis was broad, considering that the patient
had a history of cirrhosis, dyspnea, and acute
heart failure.
Portopulmonary hypertension (PoPH)
syndrome is included
within group 1 PH, (1) and accounts for 10% of the total cases of this entity.
PoPH is defined
as pulmonary arterial hypertension (PAH) associated with portal hypertension. (2) It occurs in 1-2% of these patients; (1) in fact, in the REVEAL Registry —a multicenter,
observational study on 3000 PAH patients—, the prevalence of PoPH was 5%, more common in women
and in autoimmune cirrhosis. (3) Severity is determined
by mean pulmonary pressure (mPAP) value; therefore,
it is defined as mild PoPH in patients with mPAP < 35 mmHg, and as severe PoPH in cases of
mPAP > 45 mmHg. The pathophysiology of PoPH
is not known; however, the theory
with the most significant impact states that it is due to an imbalance of vasoconstrictor mediators
and vasodilators. While most
patients are asymptomatic, dyspnea on exertion is the most
common symptom, as was the case in our patient.
Current European guidelines (1) recommend starting the diagnostic evaluation with TTE, so that,
in patients with indirect data of PH (peak tricuspid
regurgitation velocity > 2.8 m/s, RV enlargement, pulmonary artery or inferior vena cava enlargement) or with other
risk factors, right
heart catheterization would
be indicated, as was the case in our patient.
The study revealed
severe precapillary PAH: mPAP 57 mmHg,
wedge pressure 11 mmHg, elevated
transpulmonary gradient 46 mmHg, and pulmonary vascularresistance (PVR) 14.5 Wood units (WU).
Current hemodynamic diagnostic criteria for PAH include: mPAP > 20 mmHg at rest, wedge pressure 15 mmHg, and PVR > 2 WU. (1)
The ultimate criterion for diagnostic certainty of PoPH would be to confirm portal hypertension by clinical
signs; in case of doubt, venous catheterization to measure the hepatic venous pressure gradient is suggested. (4)
As this criterion was unmet in our patient, diagnosis was
"probable portopulmonary syndrome", although
isolated cases of de novo diagnosis of PoPH within the first 6 months following transplantation have been described
in the literature.
It is an entity with poor prognosis: in the absence
of therapy, PoPH has been associated with a 5-year
survival rate of 14%; (2) however, a 51% improvement in 5-year survival
rate under medical
treatment and 81% with liver transplantation have been reported.
(5) While positive
outcomes with the medical treatment of PAH have been reported, most studies are not aimed at PoPH patients
(except for the PORTICO trial,
which showed positive
hemodynamic outcomes with macitentan, or the PATENT-1 trial, (6) which included a small PoPH population under riociguat treatment, with positive functional
outcomes); in any case, this therapy has shown positive
hemodynamic and functional effects, but no effect on survival rates.
Current guidelines recommend
triple combination therapy of endothelin
receptor antagonist, phosphodiesterase-5 inhibitor and prostacyclin receptor
agonist (Class IIa recommendation) in high-risk patients,
as was the case reported
here. (1) Our patient was started on epoprostenol, sildenafil and macitentan, showing a slow but progressive improvement, followed by withdrawal of inotropes.
Typically, liver transplantation is contraindicated in these patients due to high
perioperative morbidity and
mortality, and would only be recommended in patients with liver disease per se
requiring transplantation;
it was not discussed in the case of our patient since his graft function was normal. Guidelines recommend initiation of PAH therapies
in patients with mPAP > 35 mmHg candidates for transplantation; (3) however, it is contraindicated in severe PoPH not improving with medical treatment, since perioperative mortality in patients
with mPAP > 45 mmHg is close to 100%.
One month after admission, the patient was discharged on
triple therapy and home hospitalization. Follow-up
TTE at 6 months showed normal RV function; PAH medication
was progressively withdrawn.
Differential diagnosis should consider PH associated to
high pulmonary blood flow (with normal PVR and
no need to initiate a specific therapy) and hepatopulmonary
syndrome (typically presenting without PH,
characterized by arteriovenous shunts in the pulmonary
circulation, and causing hypoxemia, orthodeoxia and platypnea; liver transplantation is the treatment of choice in severe cases).
Less common entities —which should be considered in
patients with a history of liver disease— include cirrhotic cardiomyopathy, other typical causes
of heart failure,
and extracardiac causes
of dyspnea —common in this
patient profile— such as anemia, ascites, or hydrothorax.
In conclusion, dyspnea
in patients with a history
of liver disease has been a challenge for cardiologists, not only because
of the wide range of diagnoses to be
assessed, but also because of its complex
hemodynamic profile. Portopulmonary syndrome
is a rare entity. While its standard
definition refers to patients with portal
hypertension, this entity is currently being described in already transplanted patients —particularly early, in the first 6 months
post-transplantation— as in the case
reported here; therefore, we must always take
it into account, given its poor prognosis and the absence of a specific treatment
per se.
Ana Ruiz Rodríguez1,
Uxue Idiazábal Rodríguez1, Iñigo Pereiro
Lili1
1 Department of Cardiology. Hospital Universitario de Basurto (Bilbao, Spain).
Address for reprints: Ana Ruiz Rodríguez Email: anarrmo@gmail.com
Conflicts of
interest
None declared.
(See authors’ conflicts of interest
forms on the website/ Supplementary material).
Ethical
considerations
Not applicable.
REFERENCES
1. Humbert
M, Kovacs G, Hoeper MM, et al. ESC/ERS Scientific
Document Group. 2022 ESC/ERS Guidelines for the diagnosis and treatment of
pulmonary hypertension. Eur Heart J 2022;43:3618-731.
https://doi.org/10.1093/eurheartj/ehac237
2. Navarro-Vergara
DI, Roldan-Valadez E, Cueto-Robledo G, Jurado- Hernandez
MY. Portopulmonary
Hypertension: Prevalence, Clinical and Hemodynamic Features. Curr Probl Cardiol.
2021;46:100747. https://doi.org/10.1016/j.cpcardiol.2020.100747
3. Krowka
MJ, Miller DP, Barst RJ, Taichman
D, Dweik RA, Badesch DB, et
al. Portopulmonary hypertension: a report from the
US-based REVEAL Registry. Chest. 2012;141:906-15. https://doi.org/10.1378/chest.11-0160
4. Thomas C, et al. Portopulmonary Hypertension: From Bench to Bedside. Front.
Med. 7:569413. https://doi.org/10.3389/fmed.2020.569413
5. Savale
L, Guimas M, Ebstein N, Fertin M, Jevnikar M, Renard S, et al. Portopulmonary
hypertension in the current era of pulmonary hypertension management. J Hepatol. 2020;73:130-9.
https://doi.org/10.1016/j.jhep.2020.02.021
6. Cartin-Ceba
R, Halank M, Ghofrani HA, Humbert M, Mattson J, Fritsch A, et al. Riociguat
treatment for portopulmonary hypertension: a subgroup
analysis from the PATENT-1/-2 studies. Pulm Circ.
2018;8:2045894018769305. https://doi.org/10.1177/2045894018769305