
INTRODUCTION
Adherence to statin therapy in secondary prevention of cardiovascular events remains a significant clinical challenge. Several international studies have reported a growing proportion of patients who refuse or discontinue statins, even when their medical indication is clear. This phenomenon is developing in a context where the increasing dissemination of unverified medical information further complicates this picture, particularly through social media and digital platforms. (1)
The Argentine Society of Cardiology (SAC) designed a national survey to explore the frequency and reasons for refusing statin treatment in patients with an indication for secondary prevention, according to the perception of healthcare professionals. The objective of this study is to identify the most relevant factors linked to therapeutic reluctance.
METHODS
Study design and population
A national, anonymous, voluntary survey was conducted between March and April 2025. It was distributed through the SAC's institutional registry and social media networks. The REDCap platform (Research Electronic Data Capture, Vanderbilt University, Nashville, TN, USA) was used to support the survey. (2)
Healthcare professionals from across the country were invited to participate, including physicians who treated patients in the context of secondary cardiovascular prevention. The survey consisted of closed-ended multiple-choice questions aimed at identifying the frequency, causes, and perception of changes in patient behavior.
Variables surveyed
Demographic variables were collected from respondents (specialty, region), frequency of recent refusal (last 2 months), and causes attributed to it. Respondents were also asked whether patients who refused to use statins accepted other cardiovascular therapies, and whether physicians perceived an increase in this trend.
Statistical analysis
Descriptive statistics were used to summarize the data. Categorical variables were expressed in absolute and relative frequencies (percentage). No statistical comparisons or inferences between groups were made, given the exploratory nature of the study and the absence of a formal prior hypothesis.
Ethical considerations
The study was conducted under the ethical principles of the Declaration of Helsinki.(3) Since it was an anonymous survey, with no collection of sensitive patient data or direct intervention, formal informed consent or evaluation by an ethics committee was not necessary. Participation was completely voluntary, with no financial compensation.
RESULTS
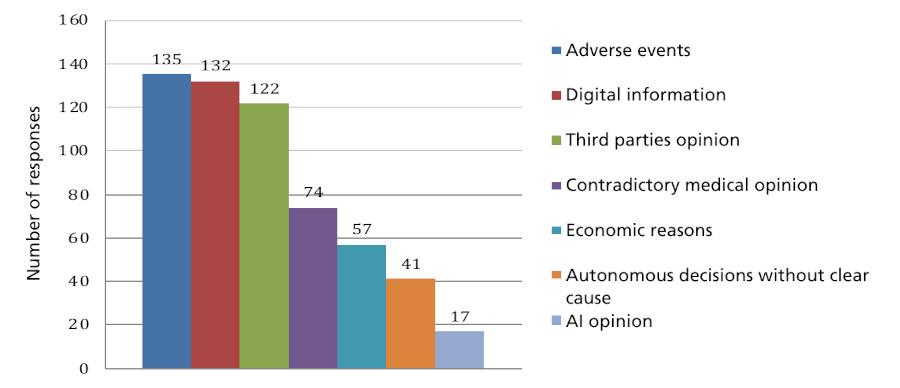
A total of 638 healthcare professionals from all regions of the country, with the exception of the province of La Pampa, responded to the survey. The majority were cardiologists (84.4%; n=538). Forty-point-nine percent (n=261) reported having received explicit refusal to use statins from patients in secondary prevention during the previous two months. The reasons most frequently cited by these 261 physicians were the occurrence of adverse events (53.4%; n=135) and the influence of negative information from digital media (50.5%; n=132). Other reasons included recommendations from family or friends (46.7%; n=122), controversial advice from another professional (28.3%; n=74), economic reasons (21.8%; n=57), and autonomous decisions without apparent cause (15.7%; n=41). A total of 6.5% (n=17) reported that the patient had consulted artificial intelligence tools as the reason for discontinuation. (Figure 1)
A noteworthy finding was that, within this 40.9% who reported having received a refusal to use statins, 74% (n=193) described having received acceptance of other cardiovascular medications. Furthermore, within that same group, 66.6% (n=174) perceived a recent increase in the frequency of treatment refusal.
DISCUSSION
The survey results reflect a worrying trend: a considerable proportion of patients with a formal indication for statins in secondary prevention refuse to start or continue treatment. Furthermore, this problem seems to be specific to this pharmacological group, as we could see that patients did not refuse the use of other drugs indicated for cardiovascular prevention in the same proportion. This behavior is often attributed to the occurrence of mild adverse events, or the fear that they will occur, and the influence of discouraging content on social media, a combination that reflects the growing digital misinformation in health.
The situation observed in Argentina is in line with international reports. In the PALM registry in the United States, 26.5% of patients with statin indication were not undergoing treatment. Within this group, 10.1% had refused to start therapy and 30.7% had discontinued it, with fear of adverse effects and perceived lack of safety being the most common reasons. (1) In Europe, studies such as EUROASPIRE V and SANTORINI reveal that less than 30-50% of patients achieved the recommended low density lipoprotein cholesterol (LDL-C) targets, despite being on treatment, (4,5) suggesting both underprescription by healthcare personnel and poor adherence by patients. In Argentina, the registry carried out by CONAREC (National Council of Cardiology Residents) in 2020 already showed that only 85.9% of patients received statins for secondary prevention, and only 30% achieved therapeutic LDL-C targets. Once again, we find the main causes in this registry to be adverse effects, fear of experiencing them, and underprescription by physicians. (6)
Despite extensive evidence on the safety of statins, there remains a marked discrepancy between perceived adverse effects and those actually observed in clinical trials. In randomized, double-blind studies, the rates of myalgia and other reported adverse effects are similar between statins and placebo, indicating that a significant proportion of symptoms attributed to treatment are not directly caused by the drug. (7) Severe myopathies with marked elevation of creatine phosphokinase (CPK) (>10 times the upper normal limit) are a rare event, with an estimated incidence of between 1 per 1000 and 1 per 10 000 patients/year, depending on the dose and predisposing factors. (8)
In contrast, in both clinical practice and observational studies, between 7% and 29% of patients report nonspecific muscle symptoms with normal or minimally elevated CPK, which contributes significantly to treatment discontinuation. (8-10) This discrepancy has been linked to the nocebo effect, demonstrated in trials such as SAMSON and StatinWISE, where more than 90% of reported muscle symptoms also appeared with placebo, reinforcing the role of expectations in the perception of adverse effects. (11,12)
On the other hand, suboptimal adherence to statins is directly associated with increased mortality and adverse cardiovascular events. In a cohort study of more than 300 000 patients, an inverse relationship between adherence and all-cause mortality was evident, reinforcing the clinical impact of therapeutic persistence. (13)
Given this scenario, it is essential to develop strategies to rebuild confidence in statins as a pillar of cardiovascular prevention. Evidence shows that multifaceted interventions, combining clinical support, personalized education, contextual adaptation, and interactive assistance, improve adherence, increase appropriate prescribing, and are associated with greater reductions in LDL-C when applied concurrently.(14) Likewise, shared decision-making, together with the use of clear and understandable visual tools, has been shown to promote a better perception of cardiovascular risk and a greater willingness to initiate and sustain therapy, an approach that is emphasized by the 2019 ACC/AHA guidelines for cardiovascular prevention. (15)
On the other hand, it is necessary to recognize the role that the digital environment plays in the construction of meanings. Evidence suggests that misinformation related to statins circulates widely on social media, where subjective experiences and negative narratives gain disproportionate visibility. Qualitative studies show that digital discourse around statins is highly polarized, with reports of perceived adverse effects influencing therapeutic decision-making. (16) In this regard, digital health literacy and the development of accessible and consistent communication tools are essential to counteract misperceptions and promote evidence-based decisions.
CONCLUSIONS
The therapeutic reluctance observed in this survey poses a real challenge for cardiovascular prevention in Argentina. Overcoming it requires a coordinated response: strengthening doctor-patient communication, promoting sustained educational interventions, using reliable digital resources, and encouraging shared decision-making. The Argentine Society of Cardiology emphasizes the need to promote actions aimed at both professionals and the community to restore confidence in essential therapies such as statins and promote informed, rational clinical decisions oriented toward comprehensive cardiovascular health care.
Conflicts of interest
Lerech Ezequiel declares an employment relationship with the companies Novartis and Gador..
(See authors' conflict of interests forms on the web).