
INTRODUCTION
Acute myeloid leukemia (AML) is a hematologic malignancy characterized by the infiltration of bone marrow, peripheral blood and, occasionally, other tissues by aberrant and abnormally differentiated clones of the myeloid lineage. (1) It accounts for 80% of acute leukemia cases in adults, and its incidence increases with age. (2)
From a clinical perspective, AML typically presents with symptoms of bone marrow failure, such as anemia, recurrent infections, or bleeding, reflecting pancytopenia. In other cases, it may present with marked leukocytosis, which can lead to hyperviscosity and leukostasis-related complications. (3)
Although initial thrombotic manifestations are uncommon, they may occur in cases of hyperleukocytosis, presenting as neurological, pulmonary, or microvascular events. (3,4) Large-vessel arterial thromboembolic complications, such as acute lower-limb ischemia, are infrequent initial manifestations and present diagnostic and therapeutic challenges. (5,6)
The case we describe involves a patient with no significant medical history who presented with acute arterial ischemia as the initial manifestation of AML. This clinical presentation is exceptional and recognizing it is crucial for an early diagnosis and appropriate treatment.
The patient was a previously healthy 70-year-old man, who presented with a sudden onset of severe (intensity 9/10) pain in the right calf, accompanied by sensory impairment and fever. On physical examination, the right lower limb was cold and pale, and no distal pulses were present. These findings were consistent with acute arterial ischemia.
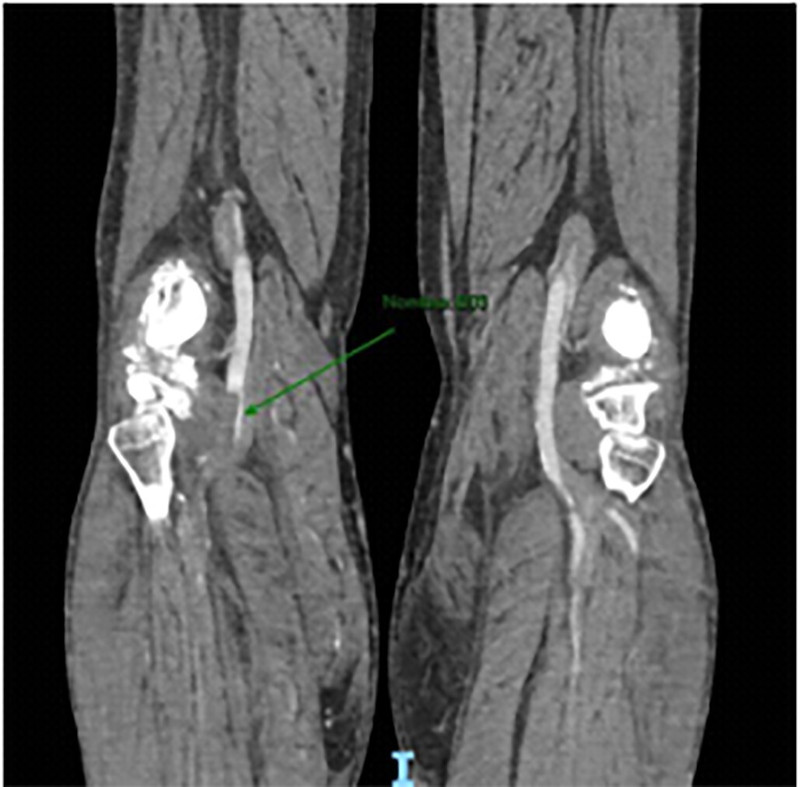
Arterial and venous Doppler ultrasound and computed tomography (CT) angiography revealed thrombosis in the distal popliteal artery extending to the posterior tibial artery, with no evidence of deep venous thrombosis.
Laboratory tests on admission revealed leukocytosis (white blood cell count 64 370/mm³, with 86% immature cells, consistent with blasts), thrombocytopenia (platelet count 47 000/mm³), mild anemia (hemoglobin 12.4 g/dL, hematocrit 37.4%), and elevated creatine phosphokinase (CPK) (1331 U/L), with no evidence of renal failure or elevated transaminases.
Given the suspicion of AML, consultation with hematology experts was sought, who ordered a bone marrow aspiration and biopsy. As the condition progressed, an initial hybrid therapy was performed. This consisted of fluoroscopy-guided thrombectomy using a Fogarty catheter and balloon angioplasty in the popliteal artery, where an atherosclerotic plaque was identified. Intraoperative angiography (Figure 1) showed the following: - Occlusion of the popliteal artery.
-
Occlusion of the anterior tibial artery, not suitable for revascularization.
-
Occlusion of the peroneal artery with poor distal blood flow.
-
Occlusion of the posterior tibial artery with inadequate recanalization.
-
Oclusión de tibial posterior con recanalización insuficiente.
Thromboembolectomy was performed on the femoropopliteal and tibial axes, achieving satisfactory technical outcomes and initial clinical improvement. However, due to early reocclusion, a repeat procedure involving multilevel arteriotomy and extensive thromboembolectomy was necessary.
The following day, the patient suffered an ischemic stroke, as confirmed by magnetic resonance angiography. This was attributed to AML. Meanwhile, the affected limb progressed to necrosis with recurrent obstruction on Doppler ultrasound, so an infracondylar amputation was performed (Figure 2). (Figura 2)

In the immediate postoperative period, the patient remained stable. However, 48 hours later, he developed a surgical wound infection and was treated with piperacillin-tazobactam and vancomycin. Seventy-two hours after the onset of symptoms, the patient suffered a cardiorespiratory arrest and died.
The case was interpreted as AML with multiple arterial thrombotic events mediated by hyperleukocytosis and leukostasis, resulting in a fatal outcome despite the multidisciplinary approach.
Arterial ischemia at the onset of AML is rare and has only been documented in isolated reports. (5,6). The disease usually presents insidiously with constitutional symptoms, hemorrhages or pancytopenia. (1,2)
The pathophysiology is multifactorial. Leukostasis involves microvascular obstruction caused by the accumulation of blasts, resulting in hypoperfusion and secondary thrombosis. (3) Aunque clásicamente se asocia a recuento leucocitario >100 000/mm3, la adhesividad celular y la interacción con el endotelio permiten su aparición con cifras menores. (3) En este caso, con 64 370 leucocitos/mm3 y 86 % de blastos, probablemente ocurrió un fenómeno de microleucostasis.Although it is classically associated with a leukocyte count >100 000/mm³, cellular adhesion and the interaction with the endothelium allow it to occur even at lower counts. (3) In this case, with a leukocyte count of 64 370/ mm³ and 86% blasts, the “microleukostasis phenomenon” (leukostasis in microvessels) likely occurred.
In addition, AML induces a systemic prothrombotic state through multiple mechanisms, including tissue factor expression in blasts, cytokine release, endothelial activation, and platelet dysfunction. This leads to arterial and venous thrombosis, which is a different phenomenon from atherothrombosis or cardiogenic embolism. There are reports of thrombi predominantly composed of blasts. (4)
The literature reflects the uncommon and severe nature of this condition. A systematic review identified 26 cases of arterial ischemia in acute leukemia over four decades, with approximately half occurring in AML. Amputation rates were 30%, and 30-day mortality was high. (5) Case reports, such as that of Kafetzakis et al., have documented femoral thrombosis without underlying atherosclerosis, attributing it to leukostasis and the intrinsic hypercoagulability of the disease. (6)
Management requires an emergency multidisciplinary approach. Alongside vascular surgery, immediate measures to treat hematologic malignancies, such as leukapheresis and induction chemotherapy, must be promptly initiated to reduce the tumor burden and improve perfusion. (3
In conclusion, AML may initially present with atypical symptoms, such as acute arterial ischemia of a lower limb. This case emphasizes the importance of considering a wide range of potential diagnoses in cases of sudden ischemia in previously healthy patients with no cardiovascular risk factors. Identifying AML as an underlying cause of arterial events enables timely referral to hematology specialists and the initiation of specific treatment. The case also highlights the importance of interdisciplinary collaboration among different departments, such as Emergency, Vascular Surgery, Intensive Care, and Hematology, to achieve an accurate diagnosis and optimize therapy.
Conflicts of interest
None declared. (See conflicts of interest forms on the website).
Ethical considerations
Not applicable