
Papillary muscle rupture (PMR) is a rare but life-threatening mechanical complication, typically after acute myocardial infarction (AMI) or infective endocarditis. (1) In the reperfusion era, it occurs in 1-5% of AMI patients, with up to 50% mortality within 24 hours of complete rupture. (1) It usually develops within the first week, particularly following an inferior AMI, causing abrupt, severe and acute mitral regurgitation (AMR), pulmonary edema or cardiogenic shock, if not promptly recognized. (2)
Although the classic presentation includes sudden hemodynamic collapse in a post-AMI patient, atypical features such as hemoptysis may obscure the diagnosis and delay definitive treatment, with potentially fatal consequences.
We present a challenging case of PMR with AMR complicating an AMI, initially presenting with pulmonary alveolar hemorrhage (PAH) and hypoxemic respiratory failure.
A 72-year-old male with hypertension and low-burden smoking presented with a one-week history of progressive dyspnea and fatigue. On the day of admission, he developed hemoptysis, prompting medical evaluation.
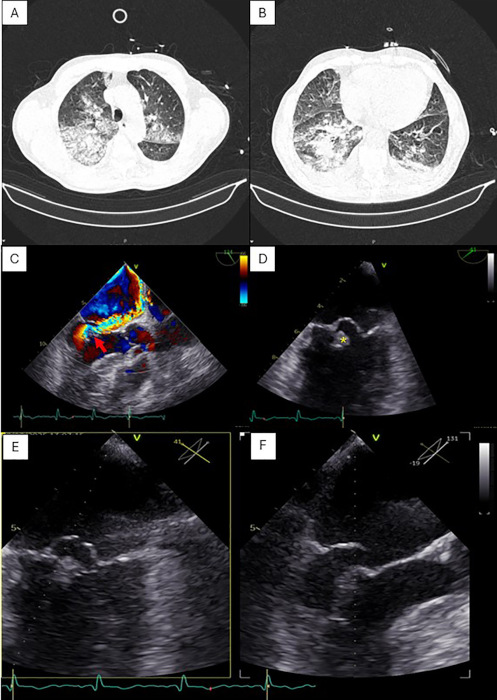
Chest computed tomography (CT) revealed diffuse bilateral ground-glass opacities and crazy-paving pattern, predominantly in the right lung, interpreted as either pneumonia or diffuse PAH (Figure 1A-B). He was initially admitted with suspected pneumonia and empirically started on antibiotics, but rapidly deteriorated with acute hypoxemic respiratory failure, requiring immediate intubation and invasive mechanical ventilation.
Laboratory testing showed markedly elevated high-sensitivity troponin I (17 062 ng/L) and ECG revealed sinus rhythm with new-onset Q waves in inferior leads, absent in prior tracings. Coagulation and liver function tests were within normal limits.
Transthoracic and transesophageal echocardiography (TEE) demonstrated preserved left ventricular systolic function with mid-basal inferoposterior hypokinesia, alongside severe, eccentric AMR, with pulmonary vein flow reversal, due to flail of the posterior mitral leaflet, involving P1-P2 scallops, consistent with probable posteromedial PMR (Figure 1C-F). A descending thoracic aortic atherosclerotic plaque with suspected mural thrombus was also noted, later confirmed with CT angiography, along with multiple splenic infarcts. (Fig.2).
Fig. 1
Chest CT scan (A-B) showing diffuse bilateral ground-glass opacities and a crazy-paving pattern, consistent with pulmonary alveolar hemorrhage. Transesophageal echocardiography demonstrating severe eccentric mitral regurgitation (red arrow) through Color Doppler imaging (C) due to flail of the posterior mitral leaflet (P1-P2 scallops), consistent with posteromedial papillary muscle rupture (yellow asterix) (D). Multiplanar views of posterior mitral leaflet flail (E-F).
These findings supported the diagnosis of inferior AMI, complicated by PMR with AMR, presenting as PAH and respiratory failure. Given the critical condition, cardiothoracic surgery team prioritized stabilization and hemorrhage control, before surgical intervention.
Within six hours, the patient developed acute ischemia of the right lower limb, with CT angiography confirming 56 mm right superficial femoral artery occlusion. Given the suspicion of systemic embolization, brain CT revealed a large right occipito-temporal infarct with mass effect and midline shift.
Due to hemorrhagic risk, anticoagulation was initially withheld. Following multidisciplinary reassessment, unfractionated heparin and acetylsalicylic acid were initiated, monitoring for hemoptysis or instability.
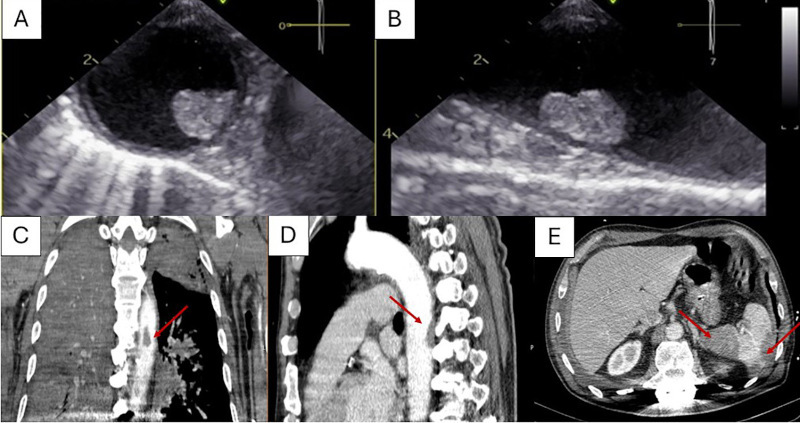
Fig. 2
Transesophageal echocardiographic images of the descending thoracic aorta demonstrating an atherosclerotic plaque with suspected mural thrombus (A) short-axis view; (B) long-axis view. Contrast-enhanced chest CT scan in coronal (C) and sagittal (D) planes revealing an atherosclerotic plaque in the descending thoracic aorta with an adjacent non-enhancing area along the posterior wall, suggestive of a mural thrombus (arrows). Multiple splenic infarcts are also visible (E).
Following stabilization, the patient was transferred to a tertiary center for further multi-disciplinary evaluation. On arrival, revascularization was deemed non-beneficial due to irreversible cyanosis of all toes and surgical candidacy for mitral valve intervention depended on neurological evolution and prognosis.
Brain magnetic resonance imaging (MRI) confirmed extensive infarcts involving the entire left middle cerebral artery territory with thrombus in M1 segment, as well as infarcts in the right posterior cerebral artery territory, with thrombus in P1 segment.
Given the catastrophic neurological prognosis and persistent multisystem involvement, surgical intervention was deemed futile and the patient died shortly thereafter.
This case illustrates critical aspects of the clinical course and management of PMR, particularly when the presentation deviates from the classic pattern. The initial picture mimicked pneumonia with diffuse PAH, delaying recognition of a mechanical complication. The absence of prior cardiac symptoms and predominant respiratory presentation highlight that PMR may develop with progressive dyspnea, preceding hemoptysis, which became the dominant clinical feature, diverting attention from a cardiac cause.
PMR most commonly involves the posteromedial papillary muscle, due to its single blood supply from posterior descending artery (typically from the right coronary artery), (2) rendering it particularly vulnerable to ischemia.(1) In this patient, electrocardiographic findings and elevated troponin I confirmed an inferior AMI as the precipitating event. PMR often occurs in small infarcts (<25% of the ventricle) with poor collateral flow, where preserved ventricular function generates high shear stress on the ischemic muscle.(1)
In AMR, the left atrium is not compliant and cannot adapt to the sudden regurgitant volume, causing abrupt pressure rise, leading to pulmonary edema. (3) Although cases of PAH associated with AMR regurgitation have been reported,(4-6) massive hemoptysis is rarely described.
PAH is characterized by alveolar space bleeding, typically due to microvascular injury and commonly presents with bilateral lung involvement. (6) In AMR, unilateral right-sided pulmonary edema and hemorrhage may occur due to the posterosuperior and rightward orientation of the mitral valve, which directs the regurgitant jet toward the right pulmonary veins, (4,6) raising capillary pressure and leading to red blood cell leakage through the alveolar-pulmonary interface.
Early diagnosis of PMR is essential but challenging in the absence of classic signs. A new systolic murmur, often cited as a hallmark, may be soft or inaudible due to pressure equalization between left atria and ventricle. (3) Unilateral cases of PAH or edema can be mistaken for pneumonia, delaying diagnosis and treatment, (3) as initially suspected in this patient.
Echocardiography remains the gold standard for diagnosis, with TEE confirming leaflet flail and chordal rupture, with 92-100% sensitivity. (1,3) In this patient, TEE confirmed the diagnosis of severe AMR caused by flail of the posterior leaflet (P1-P2) secondary to PMR. The presence of inferoposterior wall hypokinesia further supported the association with inferior AMI.
Another striking feature was the occurrence of multiple systemic emboli, including splenic infarcts, limb ischemia, and extensive ischemic stroke, likely from descending aortic thrombus, further worsening prognosis. Management of thromboembolism in PAH created a therapeutic dilemma: anticoagulation was necessary but significantly increased bleeding risk.
Definite treatment requires urgent valve surgery and coronary revascularization, as medical management alone carries high mortality. (3) In this case, surgery was delayed by PAH, embolic events, and neurological injury, highlighting the challenge of balancing surgical timing, optimization of comorbid conditions, and mitigation of bleeding and thrombotic risks.
This case highlights the diagnostic and therapeutic challenges of PMR following AMI, particularly when presenting with misleading respiratory symptoms and PAH. Despite advances, mortality remains high, particularly when diagnosis is delayed or complicated by embolization, illustrating the devastating course of untreated mechanical complications.
Conflicts of interest
None declared.
(See conflicts of interest forms on the website).
Ethical considerations
The authors declare that all procedures complied with institutional ethical standards and patient data confidentiality was ensured.
Funding
This work received no public or private financial support.