
INTRODUCTION
The use of the left internal thoracic artery (LITA), also known as left internal mammary artery (LIMA), as a graft to the left anterior descending rtery (LAD) has become the gold standard in coronary artery bypass grafting (CABG), supported by robust evidence demonstrating excellent clinical outcomes and high long-term patency. (1) The demonstrated benefits of LIMA grafting have generated growing interest in the use of the right internal mammary artery (RIMA). (2) Several studies have shown that the use of one or both internal mammary arteries (bilateral internal mammary artery [BIMA]) does not significantly increase perioperative morbidity. (1-3) Furthermore, several retrospective studies and meta-analyses have suggested that the use of BIMA may be associated with improved long-term survival. (2,4-7) Despite these potential long-term survival benefits, the use of BIMA remains uncommon. Greater technical complexity and the additional perioperative risks may also have limited the widespread adoption of this technique. Furthermore, the Arterial Revascularization Trial (ART), the only randomized clinical trial comparing the use of a single mammary artery with the use of both mammary arteries, did not demonstrate a significant survival advantage during long-term follow-up. (8)
Concurrently, off-pump coronary artery bypass (OPCAB) surgery has emerged as an alternative to on-pump CABG (ONCAB) to reduce complications associated with the use of the extracorporeal circulation and to minimize manipulation of the ascending aorta. (9,10)
However, the debate over OPCAB surgery with BIMA has persisted for more than three decades. (11,12) The combination of OPCAB with BIMA offers theoretical advantages; however, its synergistic benefit remains poorly studied, with only case reports available to date. (13,14)
The primary endpoint of this study was to evaluate long-term survival in patients undergoing OPCAB with BIMA. Secondarily, the association between ventricular function, diabetic status, body mass index (BMI) and time to death was evaluated.
METHODS
Study Design and Setting
This was a single-center retrospective cohort study conducted at the Instituto Cardiovascular de Buenos Aires. The study included all adult patients (aged ≥18 years) who underwent OPCAB with BIMA between January 2003 and December 2023. This manuscript complied with STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines and was approved by the institution’s Ethics Committee. The requirement for informed consent was waived due to the retrospective nature of the study.
Participants
From the initial patient population, we excluded those who underwent emergency CABG, combined valvular or aortic surgery, CABG using venous grafts or radial artery grafts, and patients with a history of prior coronary revascularization or who underwent ONCAB. Thus, the final cohort consisted of patients who exclusively underwent OPCAB with a BIMA T-graft configuration. To ensure complete arterial revascularization, only patients with two- or three-vessel coronary artery disease, defined as >70% stenosis in each affected territory, were included, and these patients received at least one mammary artery graft per diseased territory.
Surgical procedure
In 2002, with the availability of commercial cardiac stabilizing devices, off-pump CABG began to be used. From 2003 to the present, complete OPCAB using a BIMA T-graft configuration has been implemented. The mammary arteries were harvested using the skeletonization technique. The LIMA was anastomosed to the LAD, while the RIMA was connected as a T-shaped free graft to the LIMA, and then, sequentially, anastomoses were performed to the circumflex artery (Cx) and the distal right coronary artery (RCA). The RIMA anastomosis was located on the anterior surface of the LIMA, at the level of the left atrial appendage. All procedures were off-pump. Anastomosis quality was assessed by transit-time flow measurement (TTFM) and Doppler probes using the VeriQ system (Medistim, Oslo, Norway).
Data collection and variable definitions
Information on age, sex, BMI, diabetes, left ventricular ejection fraction (LVEF), and other baseline variables, as well as details of the surgical procedure, were obtained from the institutional electronic medical record (EMR).
For long-term follow-up, survival and the occurrence of major adverse cardiovascular events and other major postoperative complications were evaluated, including: 1) acute kidney injury, 2) stroke, 3) perioperative myocardial infarction, 4) mediastinitis, and 5) reoperations. Follow-up data were obtained from a review of electronic medical records, direct communication with the patient, their family members, and the treating physician, and telephone calls to confirm vital status at last known contact with the healthcare system.
Statistical analysis
Descriptive analysis of the study population was performed by calculating the mean and standard deviation for continuous variables or, in the case of non-normal distributions (assessed using the Shapiro-Wilk test), the median and interquartile range (IQR). Categorical variables were expressed as absolute numbers and percentages. To compare continuous variables between groups, the Student t test or the Mann-Whitney U test was used depending on the normality of the data; proportions were compared using the chi-square test or Fisher’s exact test, depending on whether the assumptions of expected frequencies were met. Early postoperative complications were also reported, including in-hospital mortality, myocardial infarction, respiratory failure, acute kidney injury requiring dialysis, stroke, and mediastinitis, with the number of events and corresponding proportions and 95% confidence intervals calculated using Pearson’s exact method.
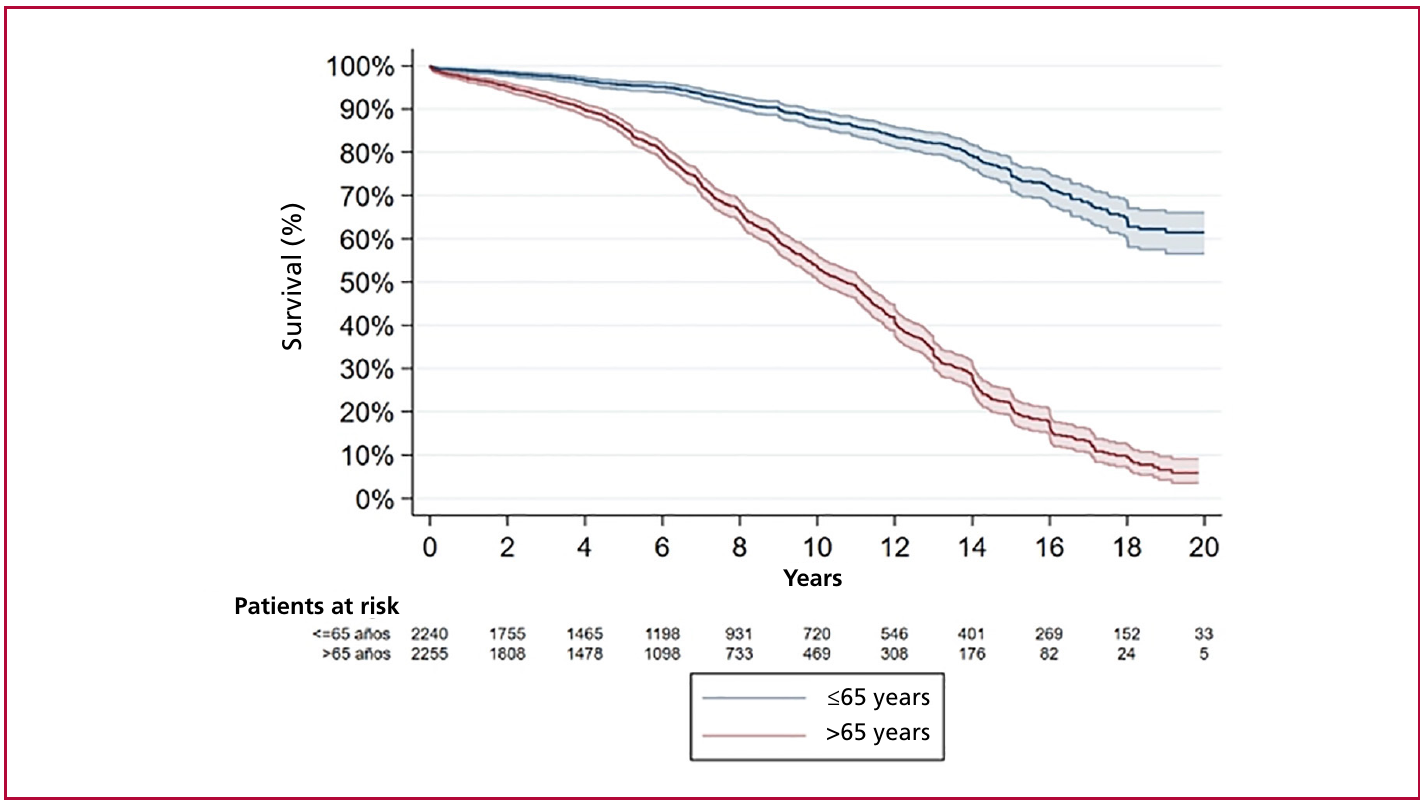
For the primary endpoint, survival at 30 days (in-hospital mortality) and at 5, 10, 15, and 20 years was estimated using survival tables graphically represented by KaplanMeier curves, with patients aged <65 years and ≥65 years presented separately. Secondarily, the association between age, BMI, LVEF, diabetes and time to death was analyzed using a Cox regression model. An unadjusted regression analysis was initially performed, followed by a regression model adjusted for potential confounders, including demographic variables (age, sex), comorbidities (chronic respiratory diseases, cerebrovascular diseases, dyslipidemia, smoking), and prior treatments (acetylsalicylic acid, calcium channel blockers, and statins). Furthermore, changes in mortality over time were assessed by comparing early mortality rates (30 days) across 5-year periods, from the beginning of follow-up in 2003 through 2023.
Finally, to assess the time elapsed until the performance of a subsequent coronary revascularization procedure, the cumulative incidence was estimated and graphically represented through curves illustrating the probability of reintervention throughout the follow-up.
Missing data were treated as completely random missing data (primarily comorbidities with a proportion of < 10% missingness). Therefore, multiple imputations were performed using the chained equation as a sensitivity analysis. Twenty imputed datasets were generated to reduce sampling error due to imputations. The proportion of missing data is presented in Table S1.
RESULTS
In the overall cohort of 4495 patients undergoing OPCAB with BIMA, the mean age was 64.1 ± 9.27 years, and 8.34% (n = 375) were women. Patients were followed for a median of 6.13 years (IQR 2.62-10.36). Fifty six percent (n = 2507) were censored (lost to followup) at 10 years and 72% (n = 3255) at 20 years. Median preoperative LVEF was 58% (IQR 50-64); 84.2% (n = 3345) had normal or mildly reduced LVEF, while 15.8% (n = 630) had moderate or severe ventricular dysfunction. The procedure was performed on an emergency basis in 42.2% of cases (n = 1884). During surgery, the total number of arterial grafts showed a median of 3 (IQR 3-4), with an average of 1 graft derived from LIMA and 2 from RIMA. Demographic characteristics and comorbidities are presented in Table 1. Inhospital mortality was 0.6% (n = 27); other in-hospital complications are presented in Table 2. Early (30-day) mortality across the study periods was as follows: 1.0% (n = 11/1153) from 2003 to 2008; 1.1% (11/967) from 2009 to 2013; 0.2% (3/1154) from 2014 to 2019, and 0.2% (2/816) from 2020 to 2023. This downward trend was statistically significant (p = 0.004).
Table 1
Characteristics of study population according to diabetes status
| Variable | All (n = 4495) | No diabetes (n = 3145) | Diabetes (n = 1350) | P | SMD |
|---|---|---|---|---|---|
| Female, n (%) | 375 (8.34) | 260 (8.27) | 115 (8.52) | 0.825 | 0.009 |
| BMI, median (IQR) | 28.0 (25.8; 30.5) | 27.8 (25.6; 30.0) | 28.7 (26.2; 31.6) | <0.001 | 0.205 |
| Age, mean (SD) | 64.1 (9.25) | 63.4 (9.51) | 65.8 (8.40) | <0.001 | 0.267 |
| Emergency surgery, n (%) | 1896 (42.2) | 1265 (40.2) | 631 (46.7) | <0.001 | 0.132 |
| Ventricular function, n (%) | 0.011 | 0.107 | |||
| Normal | 2352 (52.3) | 1678 (53.4) | 674 (49.9) | ||
| Mild | 1501 (33.4) | 1052 (33.4) | 449 (33.3) | ||
| Moderate | 416 (9.3) | 265 (8.4) | 151 (11.2) | ||
| Severe | 226 (5.0) | 150 (4.8) | 76 (5.6) | ||
| Comorbidities, n (%) | |||||
| Prior AMI | 1891 (42.1) | 1247 (39.7) | 644 (47.7) | <0.001 | 0.163 |
| Prior PCI | 1039 (23.1) | 688 (21.9) | 351 (26.0) | 0.003 | 0.097 |
| Supraventricular arrhythmia | 65 (1.45) | 44 (1.40) | 21 (1.56) | 0.792 | 0.013 |
| Carotid artery stenosis | 207 (4.61) | 133 (4.23) | 74 (5.48) | 0.083 | 0.058 |
| AAA | 46 (1.02) | 33 (1.05) | 13 (0.96) | 0.919 | 0.009 |
| COPD | 171 (3.80) | 101 (3.21) | 70 (5.19) | 0.002 | 0.099 |
| Prior stroke | 131 (2.91) | 81 (2.58) | 50 (3.70) | 0.049 | 0.065 |
| Chronic kidney disease | 283 (6.30) | 149 (4.74) | 134 (9.93) | <0.001 | 0.2 |
| Blood hypertension | 3549 (81.6) | 2359 (78.4) | 1190 (88.8) | <0.001 | 0.283 |
| Dyslipidemia | 3837 (85.4) | 2638 (83.9) | 1199 (88.8) | <0.001 | 0.144 |
| Smoking | 753 (16.8) | 571 (18.2) | 182 (13.5) | <0.001 | 0.128 |
| Type 1 diabetes | 184 (4.09) | 0 (0.00) | 184 (13.6) | <0.001 | 0.562 |
| Type 2 diabetes | 1085 (24.1) | 0 (0.00) | 1085 (80.4) | <0.001 | 2.862 |
| Heart failure | 1021 (23.5) | 768 (25.5) | 253 (18.9) | <0.001 | 0.161 |
| Unstable angina | 2200 (48.9) | 1581 (50.3) | 619 (45.9) | 0.007 | 0.089 |
| ASA, n (%) | 0.695 | 0.028 | |||
| ≤7 days | 3941 (87.7) | 2758 (87.7) | 1183 (87.6) | ||
| >7 days | 234 (5.21) | 168 (5.34) | 66 (4.89) | ||
| No | 320 (7.12) | 219 (6.96) | 101 (7.48) | ||
| Statins, n (%) | 3448 (76.7) | 2379 (75.6) | 1069 (79.2) | 0.011 | 0.085 |
| Total IMA grafts, n (%) | 0.005 | 0.038 | |||
| 2 | 733 (16.3) | 510 (16.2) | 223 (16.5) | ||
| 3 | 2635 (58.6) | 1859 (59.1) | 776 (57.5) | ||
| 4 | 1048 (23.3) | 735 (23.4) | 313 (23.2) | ||
| 5 | 79 (1.76) | 41 (1.30) | 38 (2.81) | ||
| Total LIMA grafts, n (%) | 0.577 | 0.023 | |||
| 1 | 3923 (87.3) | 2751 (87.5) | 1172 (86.8) | ||
| 2 | 572 (12.7) | 394 (12.5) | 178 (13.2) | ||
| Total RIMA grafts, n (%) | 0.473 | 0.034 | |||
| 1 | 912 (20.3) | 646 (20.5) | 266 (19.7) | ||
| 2 | 2864 (63.7) | 2009 (63.9) | 855 (63.3) | ||
| 3 | 719 (16.0) | 490 (15.6) | 229 (17.0) | ||
AAA, abdominal aortic aneurysm; AMI, acute myocardial infarction; ASA, acetylsalicylic acid; BMI, body mass index; COPD, chronic obstructive pulmonary disease; IMA, internal mammary artery; IQR, interquartile range; LIMA, left internal mammary artery; PCI, percutaneous coronary intervention; RIMA, right internal mammary artery; SD, standard deviation; SMD, standardized mean difference
Table 2
Postoperative complications according to diabetes status
| Variable | T otal (n = 449 5) | No diabetes (n = 3145) | Diabetes (n = 1350) | P |
|---|---|---|---|---|
| In-hospital mortality, n (%) | 27 (0 .60) | 20 (0.64) | 7 (0.52) | 0 .7 98 |
| Heart failure, n (%) | 41 (0 .91) | 23 (0.73) | 18 (1.33) | 0 .0 76 |
| Reoperation for bleeding, n (%) | 69 (1 .55) | 57 (1.83) | 12 (0.90) | 0 .0 31 |
| Hemodynamic complications, n (%) | 375 (8 .34) | 261 (8.30) | 114 (8.44) | 0 .9 18 |
| Acute myocardial infarction, n (%) | 47 (1 .05) | 35 (1.12) | 12 (0.90) | 0 .6 09 |
| Atrial fibrillation, n (%) | 552 (1 2.3) | 360 (11.5) | 192 (14.2) | 0 .0 11 |
| Acute kidney injury requiring dialysis, n (%) | 34 (0 .76) | 21 (0.67) | 13 (0.96) | 0 .3 92 |
| Neurological complications, n (%) | 51 (1 .13) | 29 (0.92) | 22 (1.63) | 0 .0 57 |
| Stroke with sequelae, n (%) | 12 (0 .27) | 8 (0.25) | 4 (0.30) | 0 .7 63 |
| Mediastinitis, n (%) | 53 (1 .18) | 23 (0.73) | 30 (2.22) | <0 .0 01 |
| Respiratory failure requiring MV, n (%) | 65 (1 .46) | 51 (1.63) | 14 (1.05) | 0 .1 73 |
MV: mechanical ventilation
Overall survival was 70% (95% CI 68-72%) at 10 years and 31% (95% CI 28-34%) at 20 years.
In the age-stratified survival analysis, patients aged ≤65 years had a 5-year survival of 95.8% (95% CI 94.7-96.6), 10-year survival of 87.8% (95% CI 85.889.6), and 20- year survival of 60.8% (95% CI 55.665.7). In patients aged >65 years, 5-year survival was 86.2% (95% CI 84.5-87.7), 10-year survival was 54.1% (95% CI 51.2-56.9), and 20-year survival was 5.7% (95% CI 3.4-8.9). Age >65 years was an independent predictor of mortality (adjusted HR, 4.99; 95% CI 4.33-5.75; p <0.001)
In unadjusted Cox analyses, moderate ventricular dysfunction was associated with an increased risk of death (HR 1.43; 95% CI 1.18-1.72; p <0.001), as was severe dysfunction (HR 2.38; 95% CI 1.91-2.96; p <0.001). After adjustment for covariates, the corresponding HRs were 1.22 (95% CI 1.00-1.49; p = 0.049) and 2.21 (95% CI 1.74-2.80; p <0.001), respectively. For diabetes as the primary exposure, the unadjusted HR was 1.47 (95% CI 1.30-1.66; p <0.001) and the adjusted HR was 1.30 (95% CI 1.15-1.47; p<0.001). In the subgroup analysis of diabetes and obesity (reference: non-diabetic, non-obese individuals), obese non-diabetic patients had an unadjusted HR of 0.84 (95% CI 0.71-0.99; p = 0.039) and an adjusted HR of 1.05 (95% CI 0.88-1.24; p = 0.605); non-obese diabetic patients had an unadjusted HR of 1.58 (95% CI 1.37-1.82; p <0.001) and an adjusted HR of 1.30 (95% CI 1.13-1.50; p <0.001); and obese diabetic patients had an unadjusted HR of 1.13 (95% CI 0.93-1.38; p = 0.214) and an adjusted HR 1.28 (95% CI 1.05-1.56; p = 0.015) (Figures 2, 3, and 4).


DISCUSSION
This study represents one of the largest published cohorts of patients undergoing off-pump CABG using exclusively BIMA grafting, with long-term follow-up (20 years). Patients undergoing this surgical technique demonstrated high long-term survival, with 60% of patients aged ≤65 years alive at 20 years. Severe ventricular dysfunction and diabetes were identified as predictors of increased mortality during followup; whereas obesity was not an independent predictor. Several observational studies and meta-analyses have suggested that the use of BIMA grafting offers greater survival compared to the use of a single internal mammary artery grafting. (15,16) The Arterial Revascularization Trial (ART) evaluated 10-year outcomes and found no significant differences in survival. However, this result has been criticized for multiple reasons: high crossover, heterogeneous techniques across centers, and a high rate of use of other arterial grafts in both groups, which diluted the differences. (17,18) The low adoption rate observed in the use of BIMA, despite its benefits, could be attributed to the complexity and prolonged duration of surgery, as well as the increased risk of complications, such as sternal wound infections.
This study reflects our experience of over 20 years of exclusively performing off-pump CABG with BIMA in a T-graft configuration, as originally described by Tector et al. (19) The adoption of this technique resulted from a progressive evolution over time, aimed at developing a low-morbidity procedure (off-pump and intraoperative extubation) using conduits with proven long-term patency (BIMA). In our initial series, we evaluated the technical feasibility, hospital outcomes, and the degree of early patency of the arterial grafts according to this configuration. (20) In the second stage, we conducted comparative studies in the group of patients undergoing CABG using a single internal mammary artery plus venous grafts: patients with off-pump CABG with BIMA had higher long-term survival. (21) We also analyzed long-term survival with the use of these two CABG techniques in patients over 70 years of age, with better outcomes in the group of patients with OPCAB with BIMA. (22) The use of off-pump revascularization allowed us to avoid aortic manipulation, reducing the incidence of postoperative complications such as stroke. A recent meta-analysis demonstrated that the risk of postoperative stroke, mortality, renal failure, atrial fibrillation, bleeding, and length of stay in the recovery room was lower with off-pump CABG with BIMA, which avoids aortic manipulation and completely eliminates traction and clamping of the ascending aorta. (23) We believe that the low postoperative mortality and morbidity observed in our series are largely attributable to this technique.
The upper age limit for the benefit from using BIMA has been a subject of debate. Mohammadi et al. recently demonstrated that the survival benefit associated with BIMA or other arterial conduits is lost in patients older than 60 years. (24) In our study, patients older than 65 years had poorer long-term survival with the use of BIMA, with age as an independent predictor. Severe left ventricular systolic dysfunction in the context of significant coronary artery disease remains a powerful predictor of poor prognosis. The randomized STICH trial has consistently reported that CABG improves survival rates and reduces cardiovascular mortality in patients with severe ventricular dysfunction. (25) Ikeda et al. reported, in a series of patients undergoing OPCAB with BIMA and severe ventricular dysfunction (mean LVEF 24.8%) followed for 10 years, low in-hospital mortality (1.65%) and improved ventricular function in 75.2% of cases. In the long-term follow-up, they identified LVEF <30% and non-use of BIMA as independent predictors of death and cardiac events. (26) In our series, severe ventricular dysfunction was identified as an independent predictor of death during follow-up, whereas moderate ventricular dyfunction was not.
Diabetes doubles the risk of cardiovascular disease, and approximately 75% of deaths in diabetic patients are due to coronary artery disease. (27) Longterm survival in diabetic patients is lower; diabetes is an independent predictor of long-term mortality after CABG. (28) Type 2 diabetes presents with a diffuse anatomical pattern of coronary artery disease with rapid progression, lesions with smaller luminal diameters, and greater extracardiac comorbidity; in this scenario, OPCAB may represent a lower-morbidity option. (29) Renner et al. reported that off-pump CABG is associated with lower mortality and better postoperative outcomes in diabetic patients when comparing 355 diabetic patients who underwent off-pump CABG and 502 who underwent on-pump CABG; the former was associated with a significantly lower 30-day mortality rate, fewer postoperative complications, and a significant reduction in mortality at 6 months and 1 year.(30) Srinivasan et al. reported in their propensity score-adjusted study that the incidence of stroke was six times higher, and the risk of renal failure was 2.3 times higher in the ONCAB group than in the OPCAB group. (31) The use of both internal mammary arteries-the arterial grafts of choice-is associated with a low need for reoperation, and when harvested using the skeletonization technique, it reduces the risk of potential deep sternal infections, particularly in diabetic patients. (32) Park et al., in a study exclusively involving OPCAB, demonstrated that diabetes was not a risk factor for either early or long-term outcomes. (33) In our study, diabetes was an independent predictor of lower long-term survival, and diabetic patients had a higher incidence of mediastinitis. To date, evidence regarding the relationship between obesity and outcomes following revascularization has yielded conflicting data. This is due, at least in part, to heterogeneous criteria for defining obesity and to variability in the assessed outcomes. Terada et al. evaluated the associations of BMI with short-, medium-, and longterm mortality after CABG in patients with varying grades of coronary anatomical risk and diabetes mellitus. There was lower medium- and long-term mortality in the group of overweight patients, but no differences in mortality in the obese groups after CABG. (34) Our study explored the interrelationship between diabetes and BMI, and their impact on long-term survival. Patients with diabetes had a higher risk of long-term mortality, regardless of BMI. In contrast, the group without diabetes but with a BMI ≥30 had a lower risk of mortality; this phenomenon has been defined by various surgical groups as the “obesity paradox.” (35)
Study strengths and limitations
One of the principal strengths of this study is that it represents one of the largest reported cohorts of patients undergoing off-pump CABG with BIMA, thereby providing evidence on the therapeutic impact of this surgical approach. A further strength is the 20year follow-up, which enabled the evaluation of overall long-term survival and outcomes across patient groups with different baseline characteristics. Finally, the uniform surgical approach across the entire medical staff allowed the inclusion of all patients admitted with multivessel coronary artery disease, thereby reducing potential selection bias.
However, these findings should be interpreted in light of several limitations. First, this was a retrospective study without a control group. Although our previously published controlled study demonstrated improved long-term survival with this technique, the aim of this study was to report the therapeutic impact of off-pump CABG with BIMA over extended followup to identify independent predictors. The observational design provides real-world data but can only provide evidence of association rather than causation. Second, as a single-center study, the generalizability of the findings is limited. Finally, although the analyses were adjusted for available confounders, residual confounding not accounted for in our analysis cannot be excluded.
CONCLUSIONS
This study represents one of the largest cohorts of patients undergoing off-pump CABG with BIMA with a long-term follow-up of 20 years. Patients aged ≤65 years undergoing BIMA grafting had a 20-year survival rate of 60%. Regarding predictors of mortality, we observed that while moderate ventricular dysfunction and obesity were not independent predictors, severe dysfunction and diabetes were.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web).