
The method of choice for treating atrial septal defects is catheterization. (1) To occlude both atrial septal defects (ASD) and patent foramen ovale (PFO), the most commonly used devices consist of a single nitinol wire that forms two discs with a center that joins both and occupies the defect itself. This wire mesh also contains polyester, a material that promotes endothelialization of the device. Catheter manipulation within the heart, as well as the pressure exerted by the implanted device on adjacent structures, causes myocardial injury characterized by increased troponin levels in the circulation. (2) Periprocedural myocardial injury has not been shown to be clinically relevant.
The treatment of ASD and PFO has similarities and some differences. The waist of the device used is different: it is 4-5 mm in PFO occluders, while in ASD closure devices it varies according to the size of the defect (between 8 and 38 mm), depending on the manufacturer. The ASD closure procedure may be slightly more complex in some cases, for example, the use of a balloon to measure the defect or the need to replace the device due to implant failure.
We conducted a retrospective and analytical study to compare troponin T concentration after PFO versus ASD closure procedures.
Patients undergoing percutaneous treatment of interatrial septal defects (PFO and ASD) between July 2020 and March 2025 were included in the study. Additionally, inclusion required an ultrasensitive troponin T measurement after percutaneous treatment to determine the presence of myocardial injury. Two groups were formed. The patent foramen ovale group (PFO-G) included patients treated for PFO with devices measuring 26 mm and 30 mm diameter discs and a small waist (Figure 1). In these patients, the disc size to weight ratio was 0.26 to 0.52.
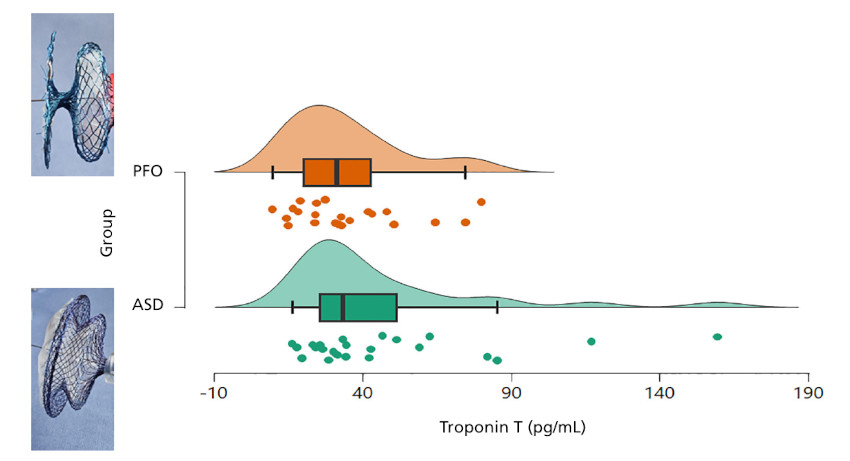
Fig. 1.
Box plot. Ultrasensitive troponin T 6 hours after completion of the percutaneous intervention. Patent foramen ovale (PFO). Atrial septal defect (ASD).
The ASD group (ASD-G) consisted of all patients with ASD closure devices in which the disc size to weight ratio was within the same range as in patients treated for PFO.
Myocardial injury was defined as an increase in ultrasensitive troponin T above the 99th percentile without signs or symptoms of myocardial ischemia. Ultrasensitive troponin T was measured 6 hours after the completion of cardiac catheterization and its reference limit was 14 pg/mL.
The study was conducted in accordance with the standards for research involving human subjects established by the Ministry of Health of the Argentine Republic (Resolution 1480/2011) and the Declaration of Helsinki. Patients' identities and personal data were anonymized.
A total of 47 patients were included in the study, with median age of 41 years and interquartile range (IQR) 26-49, 25 of whom were women (53.2%). There were 22 patients in the PFO-G, with a median age of 46.5 years (IQR 41.2- 51.5), and 25 patients in the ASD-G, with a median age of 27 years (IQR 14-45). The table shows baseline characteristics of each group. Patients in the ASD-G were treated for right chamber dilation and/or symptoms, and patients in the PFO-G were treated for cryptogenic ischemic stroke or transient ischemic attack.
Table 1.
Population characteristics
| Variables | PFO group n= 22 | ASD group n= 25 | p value |
|---|---|---|---|
| Age (years), median (IQR) | 46.5 (41.2-51.5) | 27 (14-45) | < 0.001 |
| Female gender, n (%) | 12 (54.5) | 13 (52) | 0.861 |
| Weight (kg), median (IQR) | 72.5 (65-86) | 75 (68-85) | 0.822 |
| MPAP (mmHg), median (IQR) | 18 (15-21.5) | 20 (18-22) | 0.104 |
| Aortic edge deficit, n (%) | 6 (24) | ||
| Flaccid posterior edge, n (%) | 11 (44) | ||
| Defect diameter (mm), median (IQR) | 13 (9-16) | ||
| Balloon measurement, n (%) | 6 (24) | ||
| Tunnel length (mm), median (IQR) | 9 (7.2-11) | ||
| Septum length (mm), median (IQR) | 23 (21-26.7) | ||
| Disc size (mm), median (IQR) | 30 (26-30) | 30 (24-33) | 0.594 |
| Disc/weight ratio, median (IQR) | 0.40 (0.32-0.42) | 0.40 (0.32-0.44) | 0.833 |
| ASA, n (%) | 11 (50) |
ASA: atrial septal aneurysm; IQR: interquartile range; MPAP: mean pulmonary artery pressure.
Patients in the PFO-G had a RoPE score of 7 points (IQR 6-7). Fluoroscopy time was 3.7 minutes (IQR 3.1-5.3) and the device disc size was 30 mm (IQR 26-30). The devices used were 26 and 30 mm, and all had a waist diameter of 5 mm. Nit Occlud PFO PFM Medical was always used. Patients in the ASD-G had a defect diameter of 13 mm (IQR 9-16); 6 patients (24%) had aortic edge deficiency and 11 (44%) had a flaccid posterior edge. In 6 cases (24%), a balloon was used to measure the defect. Fluoroscopy time was 5.2 minutes (IQR 3.7-9) and the devices implanted in the ASD-G had a waist size of 18 mm (IQR 14-20) and discs of 30 mm (IQR 24-33). In all cases, the Nit Occlud ASD-R PFM Medical device was used.
Elevation of ultrasensitive troponin T was found in all patients 6 hours after the procedure. In the PFO-G, it was 31.3 pg/mL (IQR 20-1-42.7), and in the ASD-G, 33.3 pg/mL (IQR 25.7-51.3); p=0.234 (Figure). There were no clinical complications during patient follow-up.
In all percutaneous treatments of atrial septal defects, there is some degree of myocardial injury determined by an increase in the value of ultrasensitive troponin T. Two previous studies have included and compared troponin values after percutaneous treatment of ASD or PFO and have found no significant differences between the two groups, although in these cases they were not matched for disc size or age. (2,3).
It cannot be determined which specific catheterization maneuvers could explain the presence of myocardial injury. Anatomopathological studies of patients who have suffered cardiac erosion reveal lacerations or perforations in areas of the left atrium that are not in contact with the device and are related to the manipulation of catheters within the cavity. Lacerations in the roof of the atrium or in the aorta in relation to the device discs have also been reported. (4,5) Although less frequently, cases of erosion with PFO closure devices have been found (6)
We can conclude that despite the lower technical complexity of PFO treatment, myocardial injury occurs to the same extent as in ASD treatment, although without clinical relevance.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web).
Ethical considerations
Not applicable.