
INTRODUCTION
Cardiovascular rehabilitation (CVR) is a proven intervention within the continuum of care for secondary cardiovascular prevention and risk factor management, with an impact on reducing mortality and rehospitalizations. Patients who adhere to these programs improve their functional capacity and quality of life, increase their ability to work and/or remain active, achieve greater autonomy, and, consequently, reduce the need for special care, disability, and loss of social productivity, as reflected in lower work absenteeism, lower social costs, and greater economic participation. (1-5) Despite these benefits, the implementation of CVR programs show marked heterogeneity in their global development and availability, influenced by economic, organizational, and healthcare access factors. (6-8)
In this context, the Exercise Cardiology Council of the Argentine Society of Cardiology (SAC), in conjunction with the Health Policy Division and methodological coordination and statistical analysis provided by the Research Division, undertook an updated survey of the country’s CVR centers. This initiative, known as the National Registry of Cardiovascular Rehabilitation Centers (RENACER-CV), aimed to describe the organizational characteristics, geographic coverage, human resources, modalities of care, and equipment of CVR centers, as well as to identify opportunities for improvement and regional development.
METHODS
First, the existence of CVR centers in the country was surveyed, using the previous survey conducted by the 2019 SAC Exercise Cardiology Council as a starting point, supplemented by consultations with cardiologists in each province. For the purposes of this registry, a CVR center was defined as any public or private institution that reported offering structured CVR programs based on supervised physical exercise, involving at least one healthcare professional, and intended for patients with cardiovascular disease at any stage of its progression. In an initial stage of the survey, priority was given to identifying centers that had a lead physician or medical director responsible for the program. Subsequently, and with the aim of achieving a more comprehensive characterization of the actual availability of CVR nationwide, the inclusion criteria were expanded to incorporate centers coordinated by kinesiologists or professionals from other related disciplines, even if they exclusively offered Phase IV programs. Inclusion in the registry did not involve external verification of compliance with formal accreditation criteria or international standards, and the collected information was based on self-reporting by the participating centers.
Subsequently, a descriptive cross-sectional study was conducted using a structured survey sent to institutional representatives of centers nationwide between July and August 2025. The questionnaire included questions aimed at exploring institutional characteristics, geographic coverage and regional distribution, available human resources (medical professionals, kinesiologists, physical education teachers, technicians, nursing staff, nutritionists, and mental health specialists, among others), the types of programs offered (Phase I or inpatient: early mobilization; Phase II: supervised rehabilitation; Phase III: transition or supervised maintenance; Phase IV: long-term maintenance, which begins once the supervised phases are completed), care modalities, the volume of patients treated, prevalent conditions, as well as equipment and functional assessment tools.
The data were analyzed by the SAC Research Area using descriptive statistics, including frequencies, percentages, and measures of central tendency.
Ethical considerations
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki (29) and its subsequent amendments. It was an observational, descriptive, cross-sectional study based on an institutional survey, without the collection of individual clinical data or patient-identifying information. For this reason, individual informed consent was waived. Participation by the centers was voluntary, and the data were analyzed in aggregate form, ensuring the confidentiality of the information. The protocol was reviewed and approved by the Research Area of the Argentine Society of Cardiology. RESULTS
A total of 74 centers were identified throughout Argentina. Fifty-nine complete responses were received from public and private centers, distributed as follows: the Autonomous City of Buenos Aires and the Province of Buenos Aires 69.4% (41 centers), the Central Region 10.1% (6 centers), the Cuyo Region 6.7% (4 centers), Patagonian Region 6.7% (4 centers), NOA Region (northwestern Argentina) 5% (3 centers), and NEA Region (northeastern Argentina) 1.7% (1 center). (Figure 1).
A total of 84.7% centers had permanent medical supervision during sessions, and 59.3% had kinesiologists specializing in CVR. Other professionals frequently included in the teams were physical education teachers (61%), nutritionists (55.9%), psychologists (37.2%), nursing staff (22%), and cardiac care technicians (22%).
Fig. 1
Distribution of the number of CVR centers by province.
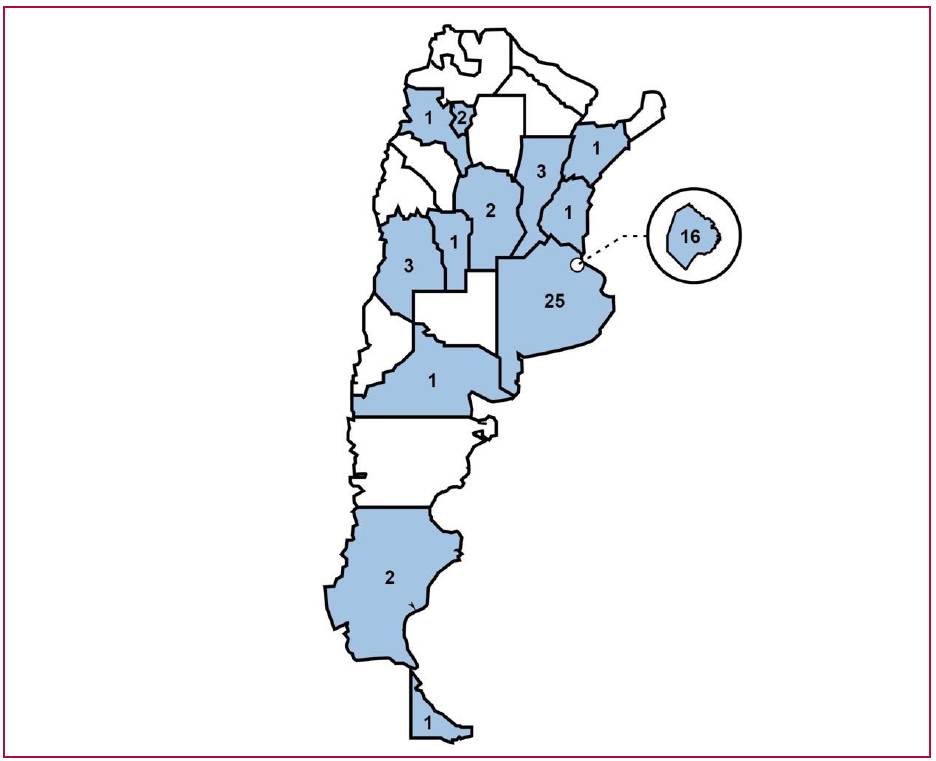
Autonomous City of Buenos Aires: Villa del Parque, Recoleta (3), Parque Chas, Caballito (3), Monserrat, Palermo (4), Balvanera, Belgrano (2) quarters; Province of Buenos Aires: Cañuelas, Ramos Mejía, El Palomar, Lomas de Zamora, Pergamino, Tigre, San Nicolás, Adrogué, Bahía Blanca (2), San Bernardo, Morón, Quilmes, La Matanza, Luján, Chivilcoy, Lanús, La Plata (2), Villa Bosch, Laprida, Ensenada, Berisso, Olavarría, San Justo; Catamarca: San Fernando del Valle; Córdoba: Villa María and Córdoba; Corrientes: Corrientes; Entre Ríos: Paraná; Mendoza: San Rafael; Río Negro: Bariloche; San Luis: Merlo; Santa Cruz: El Calafate; Santa Fe: Rafaela, Rosario (2); Tierra del Fuego: Ushuaia; Tucumán: San Miguel de Tucumán
Regarding rehabilitation phases, 79.6% of the centers (n=47) conducted Phase II programs, 93.2% (n=55) Phase III programs, and of the centers with inpatient facilities (n=30), 56% (n=17) conducted Phase I hospital-based programs.
During the COVID-19 lockdown period, 35.6% of the centers (n=21) implemented virtual CVR sessions. At the time of the survey, 13.5% (n=8) of the centers reported implementing telerehabilitation modalities.
The average annual number of patients admitted to CVR programs was 278, with marked variability among centers (range: 4-4500).
The most frequently treated conditions, expressed as a percentage of centers reporting inclusion in their programs, were coronary artery disease (96.6%), heart failure (94.9%), postoperative care following valve surgery (89.8%), patients with implantable devices (72.8%), and peripheral vascular disease (69.4%).
Regarding CVR coverage, of the 59 centers surveyed, 54.2% have a mixed coverage system. Among this group, 44.1% are private centers, funded through social welfare programs, private health insurance, and private contributions, while 10.2% are public centers that, in addition to state funding, receive contributions from social welfare programs and private health insurance. Moreover, 18.6% of the centers rely exclusively on the public health system, another 18.6% receive only private contributions from patients, 5.1% are institutions belonging to union-affiliated health insurance plans, and 3.4% of the centers did not provide information on this matter.
Most centers reported conducting structured clinical evaluations, notably the management of cardiovascular risk factors (93.2%), the admission interview (89.8%), and the exercise stress test (88.1%). Functional and nutritional assessments were available in approximately two-thirds of the centers, while direct measurement of oxygen consumption was rare (22%). (Figure 2)
Fig. 2
Monitoring practices and strategies. Values are expressed as the percentage of centers reporting implementation of each practice.
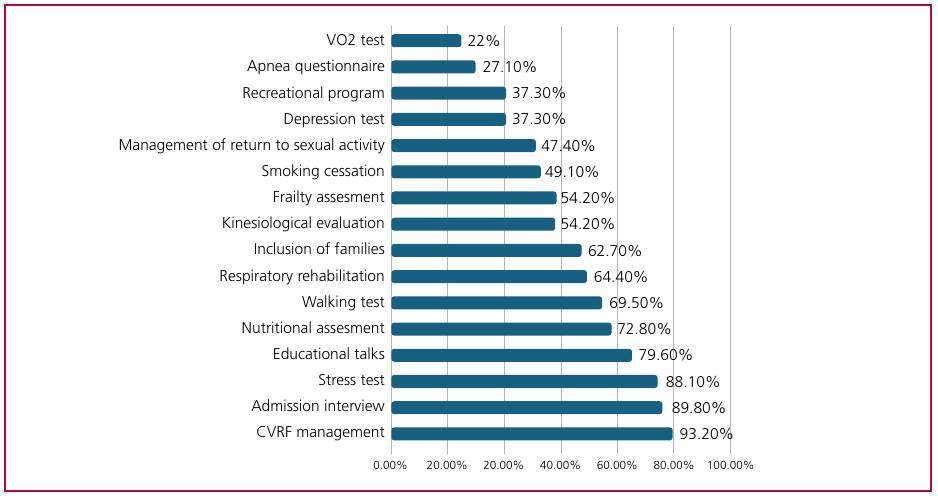
CVRF: cardiovascular risk factors; VO2: oxygen consumption.
Complementary educational and recreational interventions were implemented to a lesser extent. Among these, the most frequently reported were sports and meditation (16.9%), followed by yoga (13.5%). In contrast, practices such as tai chi and healthy cooking showed considerably lower adoption rates (3.4% and 6.8%, respectively).
Fifty-six per cent of the centers (n=33) consider essential to have a stress test (with or without imaging) before beginning exercise sessions.
DISCUSSION
The results of the RENACER-CV registry reflect a reality consistent with that described in previous national and international surveys: CVR is established as an essential and cost-effective strategy within the continuum of cardiovascular care, although significant gaps persist in its implementation and accessibility. (9-11) Accumulated evidence robustly demonstrates that CVR programs reduce mortality, improve functional capacity, and optimize quality of life in patients with cardiovascular disease, (12-14) findings confirmed by contemporary meta-analyses even in the current era of advanced pharmacological and interventional therapies. (15) In agreement, international cardiovascular prevention guidelines issue a Class I recommendation for participation in structured CVR programs. (16,17)
Unlike previous national surveys, RENACER-CV provides a comprehensive update on the state of CVR in Argentina in the post-pandemic era, incorporating for the first time systematic information on the implementation of telerehabilitation modalities and hybrid care models. In addition, the registry provides a detailed characterization of coverage and financing schemes, as well as the human resources and practices actually available at the centers- aspects of particular relevance for health planning. These elements enable not only for a description of the availability of CVR programs but also for the identification of organizational gaps and concrete opportunities for improvement in a dynamic and changing context.
As observed in other low- and middle-income countries, the registry shows a markedly unequal geographic distribution of CVR centers in Argentina, with a strong concentration in the province of Buenos Aires and the Autonomous City of Buenos Aires. The rest of the country has a significantly lower offer, with several jurisdictions lacking registered formal programs, highlighting a territorial inequity that limits effective access to this intervention, as noted in previous Latin American reports. (18,19) Characterization based on the population size of the area of influence reinforces this observation (Figure 3). The vast majority of centers (84.7%) are located in cities with more than 100 000 inhabitants, confirming that CVR remains a service strongly associated with urban settings, which have better health infrastructure and availability of specialized human resources. In contrast, the presence of centers in small cities or rural settings is minimal, representing a significant structural barrier for large segments of the population. In fact, only 1.7% of centers are located in cities with fewer than 10 000 inhabitants, and the total percentage in areas with fewer than 50 000 inhabitants does not exceed 12%. Geographic distance, difficulty in travel, and limited availability of nearby services negatively impact treatment continuity, adherence, and, ultimately, clinical outcomes.
This scenario is not unique to Argentina. In Brazil, national studies have documented marked regional heterogeneity, with a concentration of centers in urban areas and a pronounced deficit in Northen and Northeastern regions. (20,21) In Colombia, a similar picture has been described, with a predominance of programs in large cities and persistent gaps in rural and intermediate areas. (22) In Chile, although progress has been observed in integrating CVR into the public system, organizational and territorial coverage challenges persist. (23) These trends have been highlighted in regional reviews that identify insufficient funding, territorial inequity, and a lack of process standardization as common obstacles. (18)
Fig. 3
Proportion of CVR centers by population.
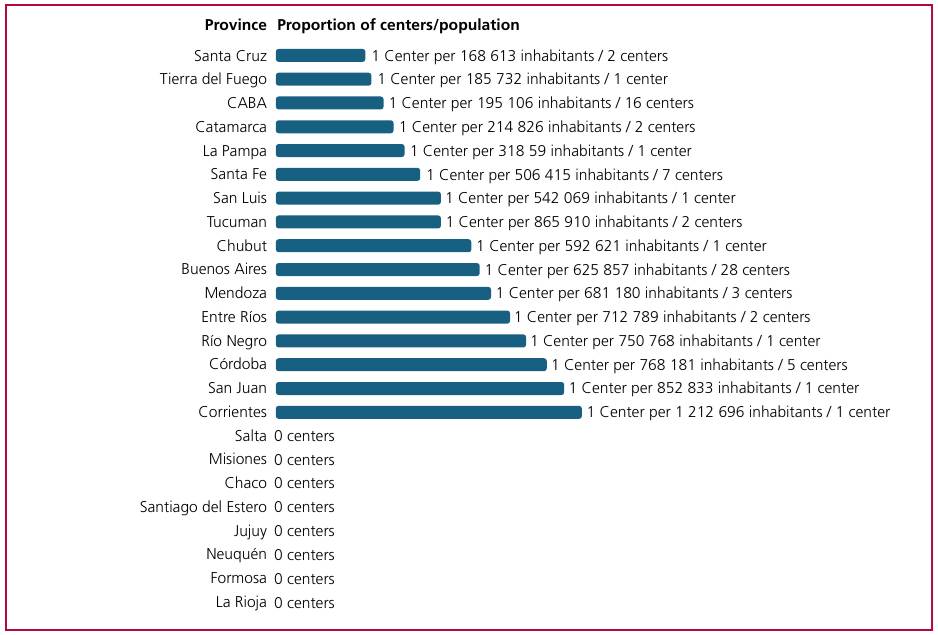
CABA: Autonomous City of Buenos Aires; CVR: cardiovascular rehabilitation
In addition to geographical barriers, economic and health coverage limitations emerge as an extra factor of inequity. Registry data indicate that the lack of health coverage is one of the main factors limiting participation in CVR programs. Patients with health insurance, private health plans, or the financial means to personally cover costs have greater access, while the offer of programs within the public system is insufficient to meet the demand of the population that depends exclusively on this subsystem. This situation reinforces the inequitable nature of access to CVR and underscores the need for health policies aimed at strengthening public provision and financing mechanisms.
Another relevant aspect identified by RENACERCV is the heterogeneity in human resources, equipment, and working modalities across centers. While a considerable proportion meets basic international standards, there is less integration of psychosocial and nutritional components-fundamental aspects for a truly multidisciplinary and patient-centered CVR. This finding agrees with those described in other regional surveys and points to a specific area of improvement. (18)
In this context, the gradual adoption of hybrid and telerehabilitation modalities emerges as a strategic opportunity. Although their current implementation is still limited, experience during the pandemic and international evidence suggest that these models can help improve accessibility, adherence, and system efficiency, particularly in countries with vast territories and significant population heterogeneity. (24-27)
From a health planning perspective, the findings of RENACER-CV provide strategic information to guide public policy decisions and health system management. The geographic concentration of centers, heterogeneity in coverage, and limited availability of programs in regions with lower population density emphasize the need to prioritize the expansion of CVR within the public system and to promote financing mechanisms that ensure equitable access. Moreover, the characterization of available resources allows for the definition of minimum quality standards and accreditation processes. In this context, as previously discussed, strengthening hybrid and telerehabilitation models emerges as a possible strategy to reduce geographic barriers and optimize resource use. The development of a coordinated national CVR network, integrated into the various health subsystems, could substantially contribute to improving cardiovascular outcomes and system efficiency. (28)
Study Limitations
It should be noted that a small percentage of centers, identified through other scientific societies of cardiology, declined to participate in the survey, which constitutes a limitation to the full representativeness of the universe of institutions. In this regard, voluntary participation and the lower inclusion of institutions not affiliated with the SAC could have generated selection biases, which must be considered when interpreting the results.
CONCLUSION
The RENACER-CV registry provided an updated and representative overview of the availability of CVR in Argentina, identifying regional patterns, territorial inequities and organizational aspects relevant to health planning.
The gradual development of a national network of CVR centers, the expansion of programs in regions with lower coverage, and the consolidation of telerehabilitation strategies are priorities for the coming years. The Exercise Cardiology Council, together with the Health Policy Area, reinforce their commitment by promoting policies, standards, and professional training initiatives aimed at improving the quality and equity of CVR in our country, and fostering collaborative networks with other cardiology societies and participants of the healthcare system, as a key strategy to promote integrated, sustainable development aligned with international recommendations.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web).