
The cardiovascular health of transgender people is now an unavoidable clinical and scientific challenge. This historically invisible population group is beginning to emerge in everyday medical practice with specific needs and risks that have not yet been sufficiently explored. In Argentina, the 2022 National Census identified 196 956 people who do not identify with the sex recorded at birth, representing 0.4% of the population in private households. (1) Far from being a marginal number, this figure reflects a growing reality that directly challenges contemporary cardiovascular medicine.
Gender affirmation therapy- a pillar of comprehensive care for transgender people- involves a multidisciplinary approach, with hormone therapy playing a central role. In the case of transgender men, testosterone administration is the treatment of choice for inducing male secondary sexual characteristics, with the aim of aligning the body with the self-perceived gender identity. (2)
However, hormone therapy is not without risks. Recent studies have documented an increase in blood pressure, a higher prevalence of dyslipidemia, insulin resistance, and an increase in the incidence of major cardiovascular events, including acute myocardial infarction and ischemic stroke, in this population. There have also been reports of erythrocytosis, changes in blood viscosity, and potential acceleration of atherosclerosis, all of which are factors that increase cardiovascular vulnerability. (3)
This scenario raises a crucial question: how can we balance the psychosocial and mental health benefits of gender affirmation therapy with the emerging cardiovascular complications? The sustained increase in the visibility of and access to these treatments has brought to the forefront the need to understand their long-term effects on coronary heart disease, classic and nonclassic risk factors, and cardiovascular morbidity and mortality.
The case we present- a trans man suffering from acute myocardial infarction- not only highlights a clinical situation unprecedented in our daily practice, but also forces us to rethink the paradigms of prevention, diagnosis, and treatment in a population whose cardiovascular vulnerability is beginning to emerge with greater clarity and urgency.
The patient is a 24-year-old transgender man with a personal history of smoking, obesity, and borderline personality disorder, with a history of problematic substance use (marijuana and cocaine). He began hormone therapy for gender affirmation with intramuscular testosterone undecanoate on a quarterly basis in 2021. Surgical history of chest masculinization. COVID-19 vaccination schedule with two doses of the Sinopharm vaccine, administered in 2020.
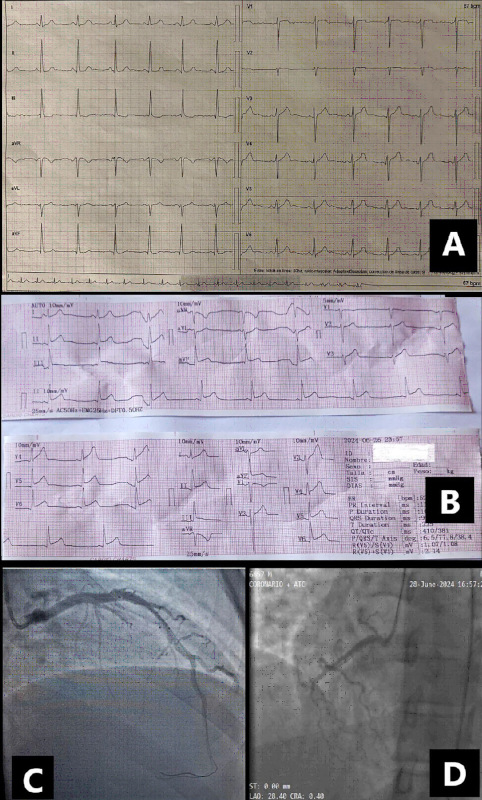
Cardiovascular disease began approximately in March 2024 with episodes of short-lived oppressive precordial pain in emotional contexts. Subsequently, he had two new episodes, so he consulted a cardiologist at an outpatient clinic in May, where he underwent an ECG (Figure 1- A) and a transthoracic echocardiogram (TTE), which showed no abnormalities, as well as a TTE with insufficient stress to show myocardial ischemia. Laboratory tests revealed testosterone levels within the male range.
On June 25, he returns to the emergency room complaining of mild typical precordial pain during physical activity. Physical examination reveals hypertension (140/90 mmHg). The ECG shows a repolarization disorder in the anterolateral and inferior walls. Ultrasensitive troponin T within normal values. A new TTE shows preserved left ventricular ejection fraction (LVEF) with no motility disorders. Admission to the pain unit is indicated, but the patient refuses. The following day, he presents with a new episode of oppressive precordial pain that begins during physical activity, lasts more than half an hour, is more intense (10/10), radiates to the jaw, and is accompanied by sweating, nausea, and belching. Physical examination reveals hypertension (160/100 mmHg) and good response to morphine analgesia. ECG unchanged from the previous day. During admission to the emergency room shock room, he presents another episode of pain with no changes in the ECG, with a lower response to intravenous analgesia, and requiring intravenous nitrites; it is decided to transfer him to the intensive care unit.
There, subepicardial injury is observed on the anterolateral and inferior walls (Figure 1- B), and it is decided to transfer him urgently to the hemodynamics room. Coronary angiography shows proximal thrombotic subocclusion of the left anterior descending (LAD) artery and distal occlusion prior to the tip (Figure 1- C). A successful primary percutaneous coronary intervention (PCI) is performed with stent implantation in the proximal segment and balloon dilatation at the distal level, and intravenous infusion of IIb/IIIa inhibitor. TTE shows slightly depressed LVEF with apical hypokinesia.
The following day, he develops precordial pain and rising troponin levels, so it is decided to transfer him back to the catheterization lab. Anterograde dissection of the right coronary artery (RCA) is observed (Figure 1- D), requiring successful primary PCI with two stents, and confirmation of LAD artery with a permeable proximal stent without lesions and no changes at the distal level compared to the previous coronary angiography.
Fig. 1.
A. Baseline ECG without abnormalities, B. Anterolateral and inferior subepicardial injury. C. Coronary angiography: left anterior descending artery with cord passage, proximal thrombus, and distal spasm. D. Dissection in the proximal segment of the right coronary artery.
Cardiac magnetic resonance imaging (MRI) shows preserved LVEF and circumferential apical transmural necrotic sequelae with akinesia and apical septal thinning (less than 5 mm) and mild aneurysmal dilatation, without thrombi, and transmural sequelae of apical segments of the right ventricle (RV) (Figure 2- A and B).
After eight days of hospitalization, the patient is discharged with antihypertensive treatment, dual antiplatelet therapy, statins, and ezetimibe. Follow-up by outpatient consultation with hematology, endocrinology, and cardiology services was recommended. During the cardiology consultation, a TTE with strain determination is performed, showing LVEF 56% (Figure 2- C and D). Approximately 20 days after the acute event, a cardiac stress MRI is performed, which reported no changes from the previous study.
Finally, after one month, laboratory results were received that rule out antiphospholipid syndrome and thrombophilia. The patient is currently under close monitoring by a multidisciplinary team with a plan to provide the best possible therapeutic strategy.
Fig. 2.
A. Cardiac MRI. T2 sequence showing biventricular edema. B. MRI with late gadolinium enhancement showing transmural septal fibrosis, lateral apical and LV apex with thinning of the apical septal myocardial thickness and mild aneurysmal dilatation without evident thrombus. Transmural sequelae of RV apical segments. C. TTE with strain evidence of apical akinesia. D. LVEF (Teicholz) 56%.

It is essential to recognize that research on the effects of hormone therapy on the cardiovascular health of transgender people is still in its early stages. (4,5) Limitations in long-term follow-up and the youth of these patients at the start of hormone therapy create a significant gap in the available evidence. However, the growing identification of disparities in emerging cardiovascular risk factors within this community compels us, as cardiologists, to face new challenges. (6)
It is crucial to emphasize the importance of cardiovascular risk stratification in this population at the start of therapy, which is not yet defined in the guidelines. Diagnostic studies such as calcium scoring, Lp(a), coronary angiotomography, arterial Doppler, etc. should be more rigorous in order to detect possible accelerated atherosclerosis at an early stage.
The impact of testosterone therapy as a cardiovascular risk factor, particularly in relation to thrombotic events and coronary artery dysfunction, requires a more rigorous approach. Its adverse effects have recently been documented, and the lack of consensus and solid evidence underscores the urgent need for further research and reports.
We must advance in this area with a multidisciplinary approach, collaborating with specialists in endocrinology, hematology, among others, to offer comprehensive and equitable medical care.
Conflicts of interest
None declared.
(See conflicts of interest forms on the website).