
In cardiology, many clinical associations have a directionality that is difficult to define. Certain variables can be both cause and consequence, generating positive feedback loops that challenge classical causality analysis.
It is assumed that a presumed cause is associated with a probable consequence by demonstrating that this association is statistically significant or, if preferred, that there is less than a 5% probability that the link is random (p< 0.05). From this perspective, it is possible to act on the cause to affect the consequence through an intervention.
In medicine in general, but in cardiology in particular, this principle supports decision-making: identifying the cause and then, through intervention, favorably modifying the consequence, improves quality of life, and reduces mortality.
Within this perspective, the association is unidirectional, from cause to effect.
But here a problem arises: statistical association does not imply direction, and although this distinction is usually irrelevant, it can be relevant under certain conditions.
"Laws of causality" have been described that, in principle, allow us to distinguish the direction from cause to effect. Although several criteria have been identified, three are of greater importance:
- temporality: the cause precedes the consequence
- biological plausibility: pathophysiological evidence supporting the direction
- intervention: removal of the cause affects the effect.
However, although they seem unquestionable, these three principles are sometimes difficult to translate into clinical practice.
UNIDIRECTIONAL OR BIDIRECTIONAL?
If a patient with no history of hypertension experiences a myocardial infarction with a critical drop in ejection fraction (cause), the neurohormonal response (consequence) is mediated by the activation of circulatory receptors and by the kidney, which, by mistakenly interpreting the pump failure as hypovolemia, induces arterial vasoconstriction and sodium and water retention, aggravating circulatory failure. (1) This is clearly positive feedback or, if preferred, a bidirectional circuit that determines the progression of heart failure (HF) (Figure 1).
Fig. 1
Diagram representing the positive feedback mechanism between HF and neurohormonal activation. HF promotes activation, which induces further myocardial damage, in a bidirectional circuit.
Figure 2 illustrates the effect of various pharmacological interventions on mortality in patients with HF. Neurohormonal blockade (renin-angiotensin-aldosterone and catecholamine inhibition) reduces mortality, calcium channel blockers are neutral, and direct vasodilators or inotropes have a negative effect. (2)
Fig. 2
Historical review of pharmacological interventions evaluated in controlled clinical trials (CCTs) for heart failure (HF) with reduced ejection fraction. Only neurohormonal blockade (renin-angiotensin-aldosterone blockade and beta-blockers) demonstrated a reduction in mortality. Calcium channel blockers, inotropic drugs, and direct vasodilators were ineffective or increased mortality. RR (CI 95%): relative risk, 95% confidence interval (personal communication, Arturo Cagide: Argentine Cardiology Congress 2010).
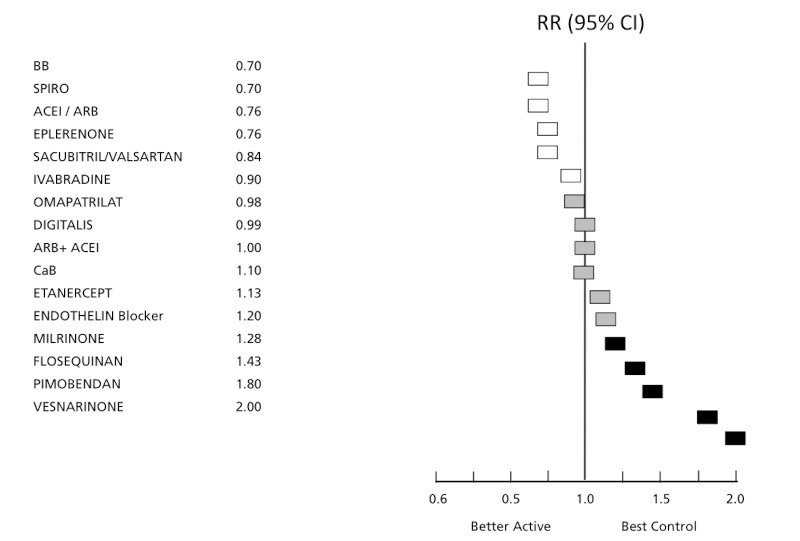
ACEI: angiotensin converting enzyme inhibitors; ARB: angiotensin receptor blockers; BB: beta blockers; CaB: calcium antagonists; Spiro: spironolactone
Thus, the benefit of neurohormonal blockade results from an intervention that acts on the consequence rather than the cause. In fact, the negative effect of direct vasodilators is a consequence of neurohormonal activation, which reinforces the above concept.
CLINICAL EXAMPLES AND BIDIRECTIONALITY
Perhaps some clinical examples will help to clarify the concept.
In arrhythmia-induced cardiomyopathy, a high heart rate (HR) secondary to supraventricular arrhythmia (cause) leads to inotropic deterioration (consequence). The severity of contractile deterioration is directly related to HR and the time of evolution. Control of HR (intervention on the cause) is associated with recovery of function some time later. (3)
However, conversely, tachycardia is often the consequence of HF, a condition that acts as the cause. In this case, catecholamine activation increases HR and inotropism, which is a compensatory mechanism for pump failure, so that the greater the circulatory deterioration, the greater the tachycardia. Clearly, in this case, the direction is opposite to that of arrhythmia-induced cardiomyopathy.
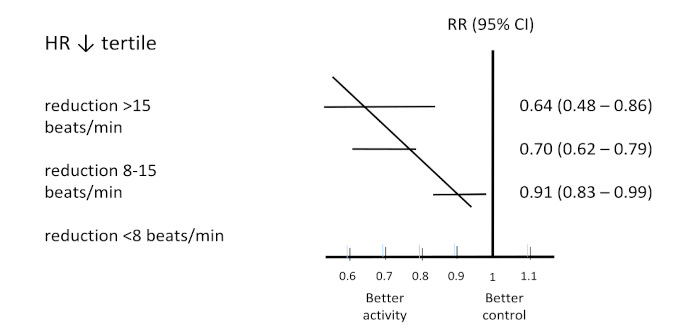
Therefore, control of HR or rhythm is one of the mechanisms associated with the benefit of beta-blockade in HF: the greater the decrease in the number of heartbeats, the greater the reduction in mortality (Figure 3). (4)
Fig. 3
Relationship between the absolute reduction in heart rate (HR) due to beta-blockers and the clinical effect expressed as relative risk (RR) of mortality. When treating tachycardia resulting from HF, the greater the reduction in heart rate, the greater the reduction in mortality. This finding is indicative of the bidirectional relationship between tachycardia and contractile damage. Adapted from (4)
Ventricular extrasystoles are in the same scenario: they are usually, but not always, a consequence of ventricular remodeling (cause), but when they reach a certain number (>10%, >20 000/day), they are a cause for the progression of myocardial damage. (5)
- The close relationship between HF and myocardial ischemia does not warrant further analysis, as their interrelationship is a common consideration in clinical practice. Delving into the pathophysiology is not the purpose of this paper, but it is clear that there is a close interrelationship and that treatment aimed at correcting both conditions has a definite impact on prognosis, regardless of which is the cause and which is the consequence.
- Left bundle branch block (LBBB) is a common complication of ventricular remodeling in cardiomyopathy. It has been found that the longer the QRS duration, the lower the survival rate, an unadjusted observational finding (Figure 4). (6) A controlled clinical trial (CCT) demonstrated that ventricular activation resynchronization improves survival by correcting the contractile dyssynchrony of LBBB (Figure 4). (7) In principle, it could be concluded that ventricular remodeling (cause) leads to LBBB (consequence), whose correction through intervention improves the progression of HF. However, it has also been demonstrated that in ventricles without functional impairment, LBBB (cause) is an independent predictor of ventricular dilation and remodeling (consequence).
Fig. 4
The left panel shows the relationship between progressive degrees of QRS width in milliseconds, with left bundle branch block morphology and survival (unadjusted observational data). Adapted from (6) The right panel shows the CARE-HF results, demonstrating the effect of resynchronization on the evolution of HF with reduced ejection fraction, where correction of dyssynchrony due to LBBB, a consequence of myocardial damage, is associated with decreased mortality. Adapted from (7)
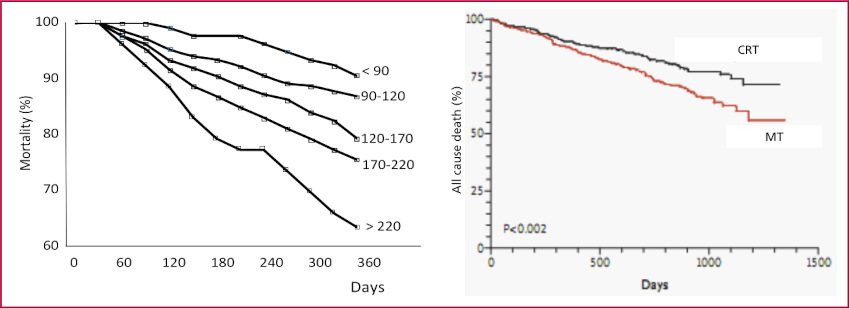
CRT: cardiac resynchronization therapy; MT: medical treatment
- In secondary mitral regurgitation (SMR), left ventricular dilation displaces the papillary muscles laterally and apically, compromising the coaptation of both mitral valves.
As suggested by its name, SMR is, as in the case of LBBB, a consequence of ventricular dilation and remodeling (cause) (Figure 5). A CCT (8) demonstrated that partial correction of mitral regurgitation through an intervention such as clipping improves SMR progression. Based on this and other studies, current valve disease guidelines recommend intervention for mitral regurgitation even when it is a consequence of ventricular failure. (9)
A second phenotype of SMR results from left atrial and atrioventricular annulus dilation, a condition frequently associated with AF (cause). In this case, the left ventricle is normal in morphology and function, with the defect being exclusively a consequence of atrial dilation (cause). Correction of SMR has been shown to be associated with improved clinical outcomes (Figure 5).
Fig. 5
The figure shows two conditions associated with secondary mitral regurgitation (SMR). On the left, SMR due to left ventricular dilation, with apical and lateral displacement of the papillary muscles (tethering) and, consequently, coaptation deficit of both valves. On the right, SMR due to atrial and atrioventricular annulus (mitral or tricuspid) dilation, usually associated with atrial fibrillation (AF) in the absence of ventricular involvement. The arrows indicate, in both conditions, the bidirectional mechanism underlying the progression of heart failure signs.
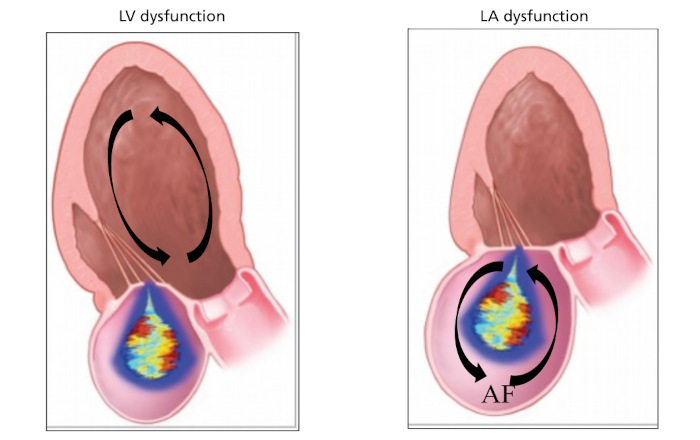
LA: left atrium; LV: left ventricle
Certainly, SMR also extends to tricuspid regurgitation in the absence of valve damage.
- Finally, the concept of bidirectionality can be extended to three clinical syndromes: diabetes (with its associated entities, hypertension, obesity, and fatty liver), heart failure, and kidney failure. Multiple epidemiological studies have demonstrated the bidirectional connection between HF and kidney failure and the unidirectional connection between diabetes and these entities. (10,11)
However, the possibility that the association between diabetes and kidney and heart disease is a positive feedback loop has been argued by various authors for some time. The concept is currently gaining interest due to its clinical relevance (Figure 6).
Fig. 6
Three conditions, heart failure (HF), kidney disease (KD), and type 2 diabetes, the latter associated with hypertension and obesity, whose association has been demonstrated in epidemiological studies. Two interventions, gliflozins and aldosterone blockade demonstrated simultaneous benefit in the three clinical syndromes, suggesting a common pathophysiological substrate and bidirectional mechanisms as determinants of progression. Secondary analyses demonstrated the effect of angiotensin II blockade.
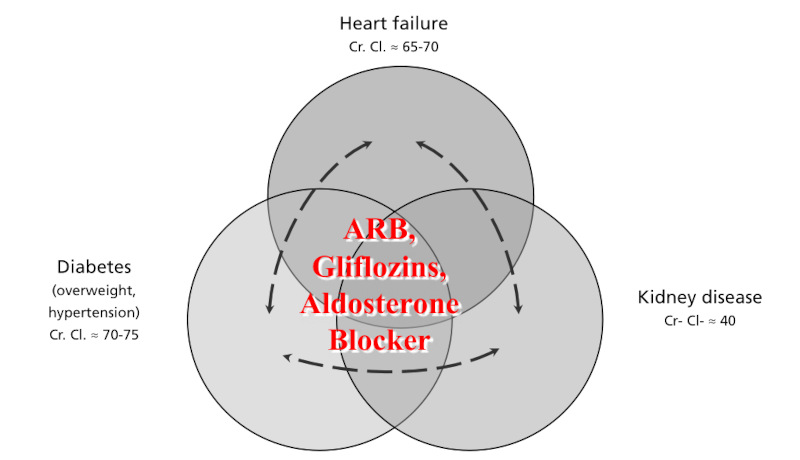
ARB: angiotensin II blockade; Cr. Cl.: mean creatinine clearance.
Numerous CCT have demonstrated, regardless of the criteria for inclusion in the trial (diabetes, HF, or kidney failure), an overall and systematic effect of gliflozins and aldosterone blockade in significantly reducing cardiovascular mortality and readmissions for heart failure, as well as in the progression of kidney failure (Figure 6).
The mechanisms of action of these drugs can be interpreted from different perspectives: from the simple treatment and prevention of hypervolemia to the inactivation of various molecular mechanisms that interact in these clinical syndromes. Moreover, it is clear that the renin-angiotensin system, inflammatory activation, insulin resistance, and oxidative stress, among others, play a central role.
The "overall effectiveness" of these drugs reinforces the concept of bidirectionality linking diabetes, HF, and kidney failure.
TEMPORALITY
Figure 7 summarizes the mutual relationship between cause and consequence in some of the clinical entities supporting this presentation.
Fig. 7
The figure summarizes various clinical conditions with their cause and consequence and the conditioning bidirectional substrate of the positive feedback mechanism determining clinical progression.
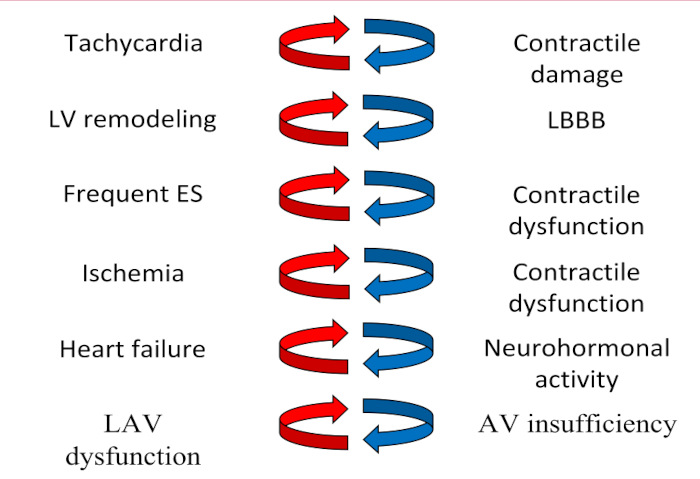
AV insufficiency: atrioventricular valve insufficiency; ES: extrasystoles; LAV dysfunction: left atrioventricular dysfunction; LBBB: left bundle branch block; LV: left ventricle
It is not only a matter of delving deeper into the blurred line between cause and consequence as a determinant of the choice of intervention, but also of advancing a concept that is sometimes difficult to transfer to clinical practice: the criterion of temporality. An example is the differential diagnosis between arrhythmia-induced cardiomyopathy and high-frequency arrhythmia secondary to HF.
CONCLUSION
The associations considered are much too complex to be summarized exclusively in terms of the link between cause and consequence and the probable positive feedback between them.
Left ventricular remodeling is only occasionally associated with LBBB or high-frequency ventricular extrasystoles, just as SMR does not occur systematically in ventricular chamber dilation. The involvement of other "individual" conditions determines the final phenotype that the clinical syndrome will adopt.
This presentation only aims to conclude that defining a variable as a consequence today does not imply its possible treatment in the immediate future. Ultimately, in the recent past, it was believed that SMR was not a treatable condition.
Ethical considerations
Not applicable.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web/Additional material).