
Takotsubo syndrome was described as a transient ventricular systolic dysfunction by Sato et al. more than 30 years ago. (1) In most cases, it has a benign course with recovery of ventricular function within weeks or months.
However, complications are reported in up to 20% of patients, the most common being heart failure, mitral regurgitation, shock, and less frequently, atrioventricular (AV) block, free wall rupture, or septal rupture. (2) We present the case of a patient admitted in our institution for Takotsubo syndrome, who developed interventricular septal rupture during the course of the disease.
The patient was a 75-year-old woman with a history of hypertension and dyslipidemia, giant cell vasculitis, and a stroke in 2021 complicated by hemorrhagic transformation.
She consulted the emergency department for oppressive chest pain of 2 hours evolution. Her blood pressure was 100/60 mm Hg and the heart rate was 70 bpm. Physical examination showed no relevant findings. An ECG performed upon admission presented ST-segment elevation in the anterior and upper lateral walls, and blood tests revealed ultrasensitive troponin T level of 866 ng/dL and N-terminal pro-B-type natriuretic peptide (NT-proBNP) of 1066 pg/mL. Given the suspicion of acute coronary syndrome, it was decided to refer her to the Hemodynamics Service on an emergency basis. Coronary angiography (CAG) exhibited coronary arteries with TIMI 3 flow and narrowing of the distal portion of the anterior descending artery, with no angiographically significant lesions. There were no signs of plaque rupture.
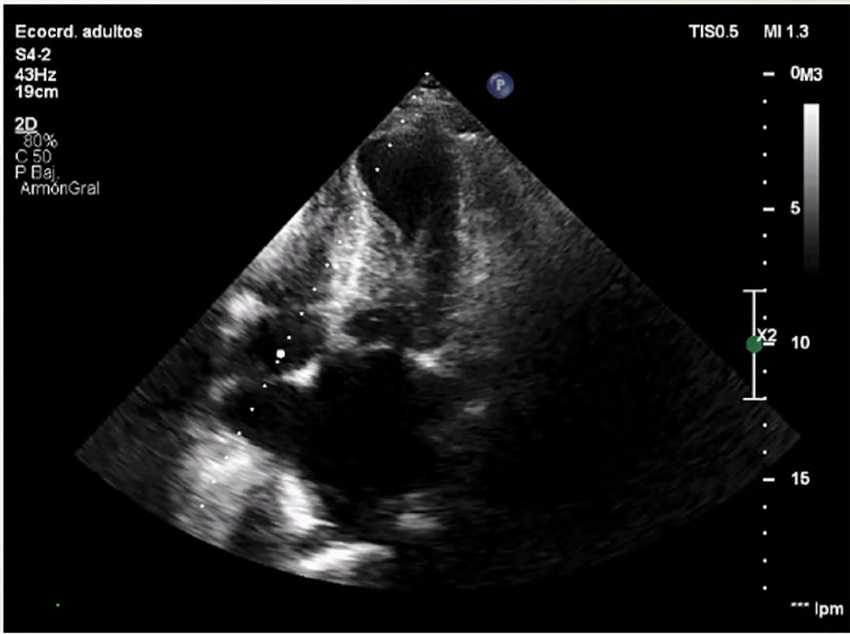
The patient's condition was stable, and she was transferred to the Coronary Care Unit, where a color Doppler echocardiogram was performed, revealing preserved left ventricular dimensions, akinesia of all apical segments, hypercontractility of the basal segments and mild to moderately reduced systolic function, with an estimated left ventricular ejection fraction (LVEF) of 45%. A mid-ventricular gradient of 45 mmHg was observed, and a pulmonary artery systolic pressure of 60 mmHg was estimated (Figure 1).
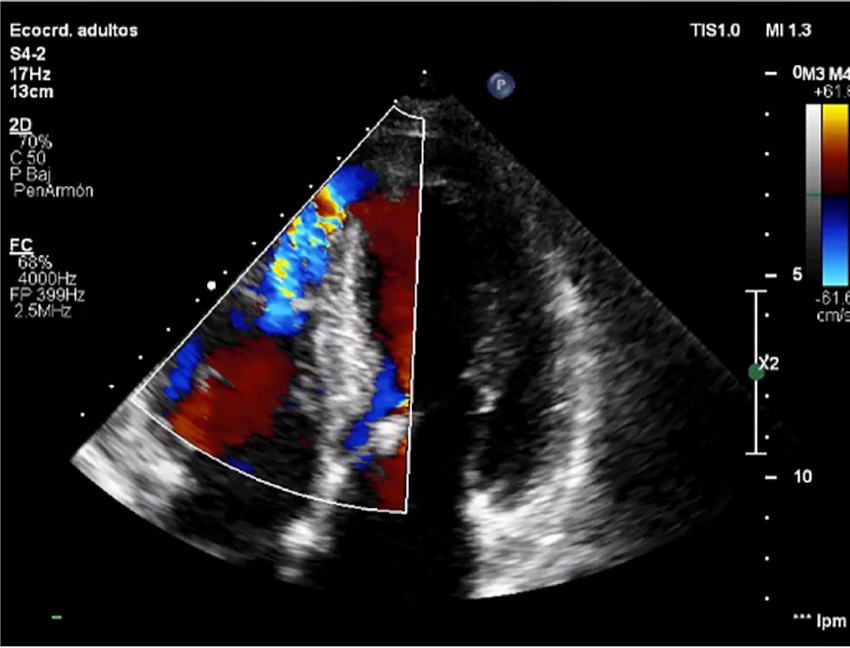
The patient remained stable until day 6, when she developed signs of decompensated heart failure. A new mesosystolic murmur at mitral focus was detected, which led to a new echocardiogram, revealing septal perforation in the apical septal segment with 12 mm diameter and 6 mm apical septum thickness (Figure 2).
After stabilization of the clinical condition with medical treatment, it was decided to proceed with surgery on the 16th day of hospitalization. The septal defect was closed with a cardiopulmonary bypass (CPB) time of 60 min and clamping time of 35 min. In the immediate postoperative period, the patient developed cardiopulmonary arrest that did not respond to resuscitation maneuvers.
Takotsubo syndrome, often associated with recent emotional or physical stress, (1) presents as transient left ventricular dysfunction, usually with hypokinesia, apical ballooning, and preservation of the basal segments.
This is usually the most common presentation, although there are atypical forms, such as the presence of left ventricular inferior or mid-ventricular hypokinesia, with increased contractility of the remaining segments.
This acute reversible cardiomyopathy mimics an acute coronary syndrome and imitates many of its characteristics, such as clinical presentation, electrocardiographic changes, and echocardiographic abnormalities.
It occurs in 90% of cases in postmenopausal women between 58 and 75 years of age.
The Mayo Clinic diagnostic criteria, modified in 2008, (3) include:
1- Acute ECG changes with ST-segment elevation or T-wave inversion with modest troponin elevation 2. Transient alteration of left ventricular contractility, dyskinesia, hypokinesia, or akinesia, with or without apical involvement, extending beyond the territory of a specific coronary artery. It is occasionally, though not always, triggered by a stressful situation
3. Absence of obstructive coronary artery disease or angiographic evidence of acute plaque rupture 4. Absence of pheochromocytoma or myocarditis.
4. Absence of pheochromocytoma or myocarditis.
In the latest review of the 2018 diagnostic criteria, the presence of significant coronary artery disease is not considered a factor excluding Takotsubo syndrome, due to the high prevalence of coronary artery disease in this patient population. (4)
The pathophysiology of this syndrome is explained by a massive catecholaminergic discharge, which in women who have lost estrogen protection has a significant impact, generating calcium overload and free radicals at the cellular level, with loss of myocardial fiber contractility, inflammation, and left ventricular apical stunning. (5)
The symptoms that usually prompt a visit to the emergency department are chest pain and dyspnea, and on the ECG, ST-segment elevation, mainly in inferior and lateral leads, with only slightly elevated troponin values. (6) The diagnosis is confirmed by Doppler echocardiography showing predominantly apical ventricular dysfunction without coronary territory involvement and CAG without angiographically significant lesions that would justify such a wall motion disorder. (4)
The vast majority of patients recover from this episode and regain ventricular function within weeks or months. As mentioned above, some patients experience complications during the course of the disease, the most common being heart failure, shock, or mitral regurgitation. Cardiac rupture is very rare, but has a high mortality rate of over 85%. The factors that predict this complication are age, female sex, high blood pressure, persistent ST-segment elevation, elevated troponin levels, impaired ventricular function, and the presence of an intraventricular gradient. The review by Zalewska-Adamiec showed that the GRACE score and basal blood glucose levels (in non-diabetics) are also associated with cardiac rupture. (6) This serious complication usually occurs between days 2 and 8 of hospitalization and is usually diagnosed by the presence of a new mesosystolic murmur. (2) The course is torpid with a high mortality rate. There are no guidelines on the best type and timing of conservative vs. surgical treatment, so individualized evaluation is recommended. (5) There is also no consensus on the adequate time of surgery. Immediate surgical intervention is recommended in cases of hemodynamic decompensation, and in all other cases, by analogy with intraventricular communication after acute myocardial infarction, it is recommended to wait at least 14 days for tissue stabilization and a better postoperative prognosis. (5) As part of the treatment, the use of beta-blockers appears to have a protective effect and improve outcomes, but more specific studies are still needed in this regard. (2) The prognosis for septal rupture is more encouraging than that for free wall rupture, since if there is no hemodynamic instability, it can be managed with medical or corrective treatment with better survival.
To date, fewer than 20 cases of septal rupture due to Takotsubo have been published, (6) and given the increased incidence of the syndrome in our society, we recommend close and careful monitoring of patients at high risk for cardiac rupture. Early detection could improve the poor prognosis and high mortality of this complication.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web).
Ethical considerations
Not applicable.