
Mobitz type I second-degree atrioventricular (AV) block, also known as the Wenckebach phenomenon, is defined as an intermittent failure of AV conduction preceded by a progressive prolongation of AV conduction time. It typically occurs in tissues composed of slowresponse cells, such as those of the sinoatrial and AV nodes. Conversely, the possibility of its occurrence in the His-Purkinje system has been overlooked and even denied, as evidenced by the limited literature available. In 1969, Rosenbaum et al. (1) described the electrocardiographic characteristics of the different forms of the phenomenon in the bundle branch system, whereas Kretz and Da Ruos experimentally demonstrated it in the divisions of the left bundle branch. (2)
We present the case of a patient whose electrocardiogram (ECG) showed a second-degree right bundle branch block interpreted as incompletely concealed Wenckebach phenomenon. (1)
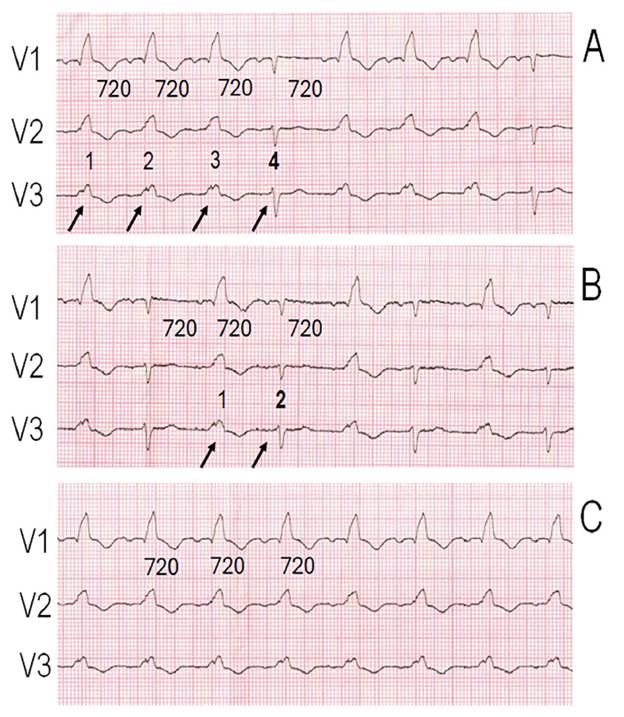
This is the case of a 64-year-old female patient with chronic Chagas cardiomyopathy, admitted for evaluation of aortic stenosis. Serial ECGs showed intermittent right bundle branch block (RBBB). Figure 1A shows regular sinus rhythm at 72 bpm and a constant PR interval of 160 ms. Beats 1, 2 and 3 display a complete RBBB pattern with a QRS duration of 160 ms. Beat 4 shows normal intraventricular conduction (QRS duration 80 ms) without preceding changes in sinus cycle length or PR interval. This sequence corresponds to a 4:3 second-degree right bundle branch block. Figure 1B, recorded with the same sinus cycle lenght and PR interval, shows 2:1 complete RBBB. Figure 1C, recorded later, shows persistent complete RBBB.
Fig. 1
A. Continuous electrocardiographic recording (V1-V3) showing sinus rhythm with a cycle length of 720 ms and a PR interval of 200 ms. At the beginning of the tracing, beats 1, 2 and 3 exhibit a complete right bundle branch block (RBBB) pattern, whereas beat 4 shows normal intraventricular conduction, constituting a 4:3 second-degree incompletely concealed Wenckebach-type block. B. With the same cycle length, 2:1 RBBB is observed. This sequence could be explained by rightward displacement of refractoriness due to contralateral retrograde activation of the right bundle branch during the beat with normal conduction. C. Persistent complete RBBB with the same heart rate and PR interval may correspond to a completely concealed Wenckebach-type block or to permanent complete block of the right bundle branch. See text for further explanation of the figures.
The Wenckebach phenomenon is a type of conduction disorder in which impulse propagation progressively slows until conduction block occurs. This phenomenon is usually observed in structures composed of slow-response cells, such as the AV node, and in pathological conditions affecting the sinoatrial node. The His-Purkinje system, composed of fast-response cells, exhibits the Wenckebach phenomenon only under pathological conditions, when fast-responses fibers acquire slow-response properties, thereby creating the substrate required for this phenomenon. (3) Rosenbaum et al. (1) described and classified the Wenckebach phenomenon in the bundle branches according to its mode of presentation into three types: 1) Direct Wenckebach phenomenon: Beginning with a beat exhibiting a narrow QRS complex and a constant sinus rate, a progressive increase in QRS duration is observed in the affected bundle branch until complete bundle branch block occurs. This is followed by a beat with a narrow QRS complex that initiates a new cycle (see Figures 2 and 6 in Reference 1). 2) Incompletely concealed Wenckebach phenomenon: This type exhibits a complete bundle branch block pattern in the beat that initiates the cycle, which remains unchanged until normalization of QRS complex occurs. The first beat of each cycle shows a complete block pattern whenever impulse delay in the affected branch exceeds 40-60 ms, corresponding to transseptal conduction time. Impulse delay increases with each beat while maintaining the same pattern until complete block of the impulse occurs, followed by a beat with normal conduction, as illustrated in Fig. 1A. Similar examples are shown in Figures 3, 4 and 7 of Reference 1. In our case, the incompletely concealed Wenckebach phenomenon was not preceded by a direct Wenckebach, unlike the cases published by Rosenbaum et al. and illustrated in Figures 2 and 6.
An essential condition for this sequence to occur is the absence of retrograde activation of the affected bundle branch or fascicle originating from the contralateral ventricle. 3) Completely concealed Wenckebach phenomenon: This occurs when conduction delay of the first beat in the cycle exceeds 40 to 60 ms, such that the QRS complex exhibits a complete block pattern, as do the subsequent beats with longer delays in impulse propagation until complete block occurs. The new cycle will consistently show complete block of the affected bundle, and the phenomenon therefore will remain concealed. Figure 1C may correspond to this type of block. This possibility is inferential and can only be suspected when preceded by either a direct Wenckebach pattern or an incompletely concealed Wenckebach pattern (Fig. 1A). In all three types of block, the PR interval remains unchanged, and a stable sinus rate facilitates interpretation. Differential diagnoses include supernormal conduction, (4) the linking phenomenon, (5) intermittent bundle branch block, (6) and Mobitz II second-degree AV block. (6)
Demonstrating the different types of bundle branch or fascicle block by means of an electrophysiological study is extremely difficult because it requires recording electrograms both proximal and distal to the site of block. Furthermore, as this practice provides no benefits for patient management, it is not recommended.
We believe that an important contribution of this case report is to highlight that the Wenckebach phenomenon is not exclusive to AV conduction, and that its occurrence within the intraventricular conduction system should be suspected on the basis of the features described in this article.
Conflicts of interest
None declared.
(See conflicts of interest forms on the website).
Ethical considerations
Not aplicable.