ORIGINAL ARTICLE
Cardiovascular Risk Profile in Women from Three
Different Areas of the Province of Tucumán, Argentina
Perfil de riesgo cardiovascular en mujeres de tres
entornos de la Provincia de Tucumán – Argentina
Damián Holownia1, Ricardo S. Galdeano1,2,
María S. Rojas Jordán1,2, Palavecino Darío Omar1,3, Abregú José Daniel1,4, Mario O. Martinengui1, Rodrigo O. Marañón1, 5, Claudio M. Joo Turoni
1
Tucumán District
– Sociedad Argentina de Cardiología
2
Sanatorio Racedo
(Monteros) – Tucumán
3
Provincial Health
System (Sistema Provincial de Salud, SIPROSA) –
Tucumán
4
Municipality
of Aguilares – Tucumán
5
Biomedical
Department, Institute of Physiology, School of Medicine, National University of Tucumán
(Universidad Nacional de Tucumán, UNT); Higher Institute of Biological Research (Instituto Superior de Investigaciones Biológicas,
INSIBIO)-National Scientific
and Technical Research
Council (Consejo Nacional de Investigaciones Científicas y Técnicas, CONICET) –
Tucumán
Address for reprints: Claudio M. Joo
Turoni. Departamento
Biomédico, Instituto de Fisiología, Facultad de Medicina, UNT; INSIBIO-CONICET.
Av.
Gral. Roca 1800, Tucumán.
Rev Argent Cardiol 2023;91:180-186. http://dx.doi.org/10.7775/rac.v91.i3.20629
ABSTRACT
Background: The role of the environment on
female population health in Tucumán has been little studied. This study aimed
to evaluate the cardiovascular risk profile in women from rural, peri-urban and urban areas in the province of Tucumán
(Argentina) and to analyse their differences.
Methods: An analytical cross-sectional study
was conducted in 3 groups of women from Tucumán: rural (n = 125), peri-urban (n = 50) and urban (n = 112).
Results: Blood pressure (BP) was
lower in the rural group; the urban group showed higher heart rate and smaller
neck circumference. Of the studied women, 29.7% were overweight and 42.4% obese, and no significant differences were found in the 3
groups. Increased neck circumference was observed in 62% of women in the rural
group, 79% in the peri-urban group and 41% in the
urban group (p <0.001). Smoking was more frequent in the urban group. In the
urban and peri-urban groups, the proportion of women
with higher education level was greater (p <0.001). Education level was
positively correlated with heart rate.
Conclusion: Regardless of the environment,
women from Tucumán are overweight or obese and have other risk factors for
cardiovascular disease. This should be considered when planning policies and
making decisions in order to improve their prognosis.
Keywords: Cardiovascular Disease - Women –
Environment
RESUMEN
Introducción:
El rol del entorno
sobre la salud en la población femenina de Tucumán está poco estudiado. El
objetivo del presente trabajo fue evaluar el perfil de riesgo cardiovascular de
mujeres de los entornos rural, periurbano y urbano de la provincia de Tucumán
(Argentina).
Material
y métodos: Se
efectuó un estudio analítico transversal en 3 grupos de mujeres de Tucumán:
rural (n=125), periurbano (n= 50) y urbano (n=112).
Resultados:
La presión arterial
(PA) fue menor en el grupo rural; el grupo urbano presentó mayor frecuencia
cardíaca y menor circunferencia de cuello. El 29,7% de las mujeres presentaron
sobrepeso y el 42,4% obesidad, sin diferencia significativa entre los 3 grupos.
La circunferencia de cuello estuvo aumentada en el 62% de las mujeres del grupo
rural, 79% del periurbano y 41% del urbano (p<0,001). El grupo urbano
presentó más frecuentemente tabaquismo. En los grupos urbano y periurbano fue
mayor la proporción de mujeres con estudios superiores (p <0,001). El nivel
educativo se correlacionó positivamente con la frecuencia cardíaca.
Conclusiones:
Independientemente del
entorno las mujeres de Tucumán presentan sobrepeso u obesidad asociados a otros
factores de riesgo para enfermedad cardiovascular. Ello debe ser tenido en
cuenta para la elaboración de políticas y la toma de conductas a fin de mejorar
su pronóstico.
Palabras
claves: Enfermedades
Cardiovasculares - Mujeres - Entorno
Received: 02/04/2023
Accepted: 05/06/2023
INTRODUCTION
Cardiovascular disease (CVD) is the leading cause of
morbidity and mortality worldwide (1) and in Argentina. (2) The so-called "social gradient" (decrease
in mortality and morbidity rates as social status increases) (3) has already been shown to
occur in a wide range of conditions, including CVD. (4)
In urban areas, population has easier access to health
services, but environmental factors, such as pollution, noise, and daily
stress, affect the cardiovascular health. (5) The peri-urban areas have
the disadvantage of being a transitional and unstable territory in terms of
social networks, which is associated with increased cardiovascular risk. (6,7) In addition, it has been conventionally described
that the prevalence of CVD is lower in rural areas. (8) However, this concept is changing, (9) since a high prevalence of
overweight was observed in different indigenous communities. (10,11) In Argentina, a 38% prevalence of metabolic syndrome
has been found in the Toba community (indigenous people living in central
Chaco). (12) More recently, we have found that the Quilmes community (rural
indigenous people living in the middle and high mountains who still preserves
pre-Inca traditions) in Tucumán has a prevalence of risk factors for CVD
similar to that in urban areas. (13)
The province of Tucumán, located in northwestern
Argentina, with an area of 22 525 km², has rural areas with difficult access,
densely populated urban areas (the capital city has 605 000 inhabitants in 91
km2) and strings of peri-urban areas surrounding the cities. In the urban and peri-urban areas of Tucumán, according to data from the
National Institute of Statistics and Censuses (Instituto
Nacional de Estadísticas y Censos, INDEC), the poverty rate was 42.7% in the second
quarter of 2022. (14) However, the impact of the environment on CVD risk
factors in women is still being studied. This view is consistent with the
worldwide literature which indicates that there is a dichotomy between real and
perceived CVD risk in women. (15,16)
This study aimed to evaluate the cardiovascular risk profile
in adult women from rural, peri-urban and urban areas
of the province of Tucumán (Argentina) and to analyse
their differences.
METHODS
An analytical cross-sectional study conducted in 3
population groups of women from different areas of Tucumán.
- Rural group: Women from Quilmes, a middle and high
mountain area where pre-Inca traditions are still preserved, who participated
in the Sonqo Calchaquí 2018
study (13) (n = 125).
- Peri-urban group: Women
from Villa Muñecas, a peripheral neighbourhood
located 3 km away from the city, who participated in a cardiovascular health
activity organized by the Argentine Society of Cardiology (Sociedad
Argentina de Cardiología, SAC), Tucuman District, on
Women's Day in March 2021 (n = 50).
- Urban group: Women living in the city of San Miguel
de Tucumán and performing desk jobs at the Municipality, who underwent a
cardiovascular health registry in September 2019 (n = 112).
In this study, the following variables were assessed:
- Age: Expressed in years.
- Education level: Expressed as completed level
(illiterate, primary school, secondary school or higher education).
- Presence of the following CVD risk factors: Smoking,
dyslipidemia, hypertension (HT) or diabetes. Women were asked about the
presence of said risk factors. A semiquantitative
score was made according to the number of risk factors mentioned (0 to 4).
- Salt added to cooked food.
- Weight (kg): It was measured with a digital scale.
- Height (cm): It was measured with a portable height
rod.
- Neck circumference (cm): It was measured with a
non-expandable measuring tape. It was considered increased when it was greater
than 34 cm. (17)
- Waist circumference (cm): It was measured with a
non-expandable measuring tape. It was considered increased when it was greater
than 88 cm. (17)
- Body mass index (BMI): It was calculated as weight
in kg/(height in m2. Women were classified
according to their nutritional status as follows: underweight (BMI <18.5);
normal weight (BMI ≥18.5 and <25); overweight (BMI ≥25 and
<30); obesity (BMI ≥30 and <35); severe obesity (BMI ≥35 and
<40); and morbid obesity (BMI ≥40).
- Systolic blood pressure (SBP) and diastolic blood
pressure (DBP) values were expressed in mmHg: It was measured with an Omron
7120® automatic digital sphygmomanometer according to the applicable
guidelines. (18) Pulse pressure (PP) was calculated as SBP - DBP and mean blood pressure
(MBP) as DBP + (PP/3).
- Heart rate and O2 saturation were measured with an An Mat® pulse oximeter.
Statistical Analysis
The results were compiled in a Microsoft Excel 2010
spreadsheet and expressed as percentage (%) or mean ± standard error, as
required. The statistical analysis was performed with GraphPad
Prism 5.02 software. Student’s t-test, ANOVA with Newman-Keuls’
post-test, Pearson’s correlation (r) or chi-square test (2) were used, as required.
Results were considered significant with a <5% probability (p <0.05).
Ethical Considerations
All participants granted the appropriate oral and
written informed consent to participate in this study.
RESULTS
The average age of the studied women was 48.9 ± 0.9
years, with no differences among the 3 groups: (rural: 50.2 ± 1.8 years, peri-urban: 47.7 ± 1.9 years, urban: 48.1 ± 1.0 years, p =
NS).
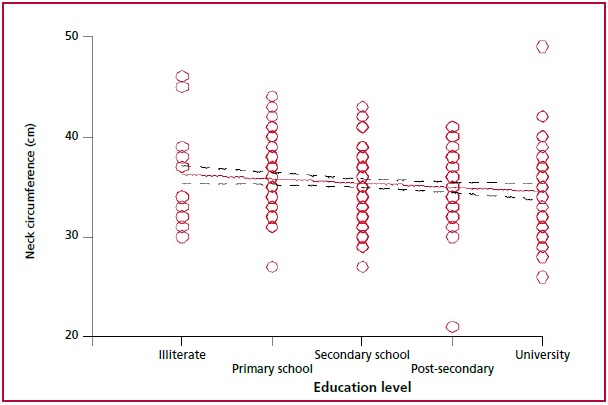
Education level of the studied women is shown in Figure 1. Illiterate women were
reported only in the rural group. The percentage of women with higher education
level was greater in the urban and peri-urban groups
than in the rural group (p <0.001).
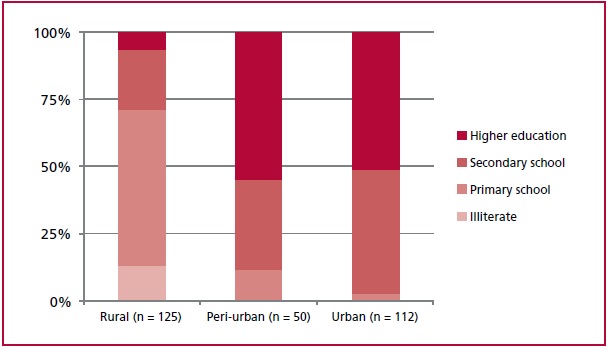
Fig. 1. Education level in the studied population.
Anthropometric and hemodynamic values are shown in Table 1. Weight and height values
were lower in the rural group than in the other two groups, but the average BMI
was elevated in all the studied population, with no differences among the 3
groups.
Table 1. Anthropometric values in the studied population
|
|
Rural (n = 125) |
Peri-urban (n = 50) |
Urban (n = 112) |
Total (n = 287) |
|
|
Weight (kg) |
68 ± 1 |
73 ± 2+ |
78 ± 2*** |
72.6 ± 1.0 |
|
|
Height (cm) |
154 ± 1 |
160 ± 1*** |
160 ± 1*** |
1.6 ± 0.1 |
|
|
BMI |
28.5 ± 0.5 |
28.5 ± 0.8 |
30.3 ± 0.6 |
29.3 ± 0.4 |
|
|
Neck circumference (cm) |
36.9 ± 0.8 |
36.1 ± 0.4 |
34.3 ± 0.4** |
35.7 ± 0.4 |
|
|
Waist circumference (cm) |
95.6 ± 1.3 |
97.9 ± 2.0 |
95.0 ± 1.8 |
95.8 ± 1.0 |
|
|
BP (mmHg) |
SBP |
123.7 ± 1.9 |
131.5 ± 2.4** |
131.2 ± 1.8*** |
128.0 ± 1.2 |
|
DBP |
75.6 ± 0.9 |
82.8 ± 1.9** |
80.7 ± 1.0** |
79.1 ± 0.7 |
|
|
PP |
44.9 ± 1.4 |
48.7 ± 2.0 |
50.5 ± 1.2** |
49.0 ± 0.8 |
|
|
MBP |
90.5 ± 1.2 |
99.0 ± 1.9*** |
97.6 ± 1.2*** |
94.7 ± 0.8 |
|
|
Heart rate (bpm) |
76.4 ± 1.2 |
78.4 ± 1.1 |
79.0 ± 1.1* |
77.6 ± 0.7 |
|
|
O2 saturation (%) |
94.9 ± 0.3 |
97.0 ± 0.2*** |
97.3 ± 0.2*** |
96.7 ± 0.2 |
|
*: p <0.05
vs. rural; **: p <0.01 vs. rural; ***: p <0.001 vs. rural; +: p <0.05
vs. urban. 0% 25% 50%
75% 100%
Neck circumference was smaller in the
urban group, but waist circumference was similar in the 3 groups. Although SBP
and DBP values, on average, remained within the normal rank, they were higher
in the peri-urban and urban groups than in the rural
group, and PP values were higher in the urban group than in the peri-urban group. Heart rate values were also higher in the
urban group, and O2 saturation was lower in the rural group.
When nutritional status was
evaluated, 27.9% of women showed normal weight; 29.7% was overweight and the
remaining 42.4% had some level of obesity (26.5% obesity; 10.6% severe obesity
and 5.3% morbid obesity). No underweight women were found. The nutritional
status distribution was similar in the 3 groups (p = NS).
Increased neck circumference was
observed in 62% of the women in the rural group, in 79% in the peri-urban group and in 41% in the urban group (p
<0.001) and increased waist circumference was observed in 69% of the studied
women, with no significant differences among the 3 groups.
The number of risk factors for CVD,
according to the semiquantitative score, was higher
in the urban group (Figure 2A). The proportion of women with no
risk factor was higher in the rural group (53%) than in the peri-urban
(44%) and urban (33%) groups (p <0.001). When each risk factor was analysed separately, HT was the most prevalent (30%),
followed by dyslipidemia (25%), smoking (23%) and diabetes (6%). The urban
group reported a higher percentage of smoker women (p <0.001). Similar
percentages for the other risk factors were found in the 3 groups (Figure 2B).
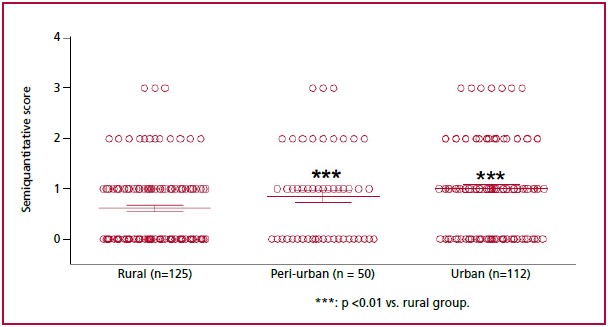
Red dots
represent each patient. Blue lines represent the mean ± standard error of each
group.
Fig. 2A. Number of risk factors for CVD in the studied groups.