
INTRODUCTION
Heart failure (HF) is a disease with high prevalence and morbidity and mortality. One of its prognostic and therapeutic challenges is hyperkalemia, which is one of the most common electrolyte disturbances in this population, with a reported incidence of up to 25%. It is classified as mild (>5.0-<5.5 mEq/L), moderate (5.6-6.0 mEq/L), or severe (>6.0 mEq/L). (1-3) Recent evidence demonstrates a U-shaped relationship between serum potassium levels and mortality in patients with HF, with increased risk at both low and high levels. (4,5)
The standard treatment for heart failure with reduced ejection fraction (HFrEF) includes drugs that act on the renin-angiotensin-aldosterone system. (6) Despite strong evidence supporting their use, a significant proportion of patients do not reach target doses, mainly due to the onset of hyperkalemia, symptomatic hypotension, or worsening renal function. (7-11)
This scenario presents a therapeutic dilemma between the long-term prognostic benefits of diseasemodifying drugs and the immediate risks associated with hyperkalemia. (12,13) The coexistence of comorbidities such as chronic kidney disease (CKD) and diabetes mellitus further increases this risk. (14-16) In this context, the present study aimed to determine the prevalence of hyperkalemia and its associated risk factors in a cohort of patients with HFrEF treated at a specialized unit in Montevideo.
METHODS
An observational, analytical, descriptive, and retrospective study was conducted including outpatients over 18 years of age with HFrEF (left ventricular ejection fraction, LVEF, ≤ 40%) treated at the Multidisciplinary Heart Failure Unit (UMIC) of Hospital de Clínicas, The study period spanned from 2018 to 2022. Patients with acute kidney injury and stage D HF were excluded.
Definition of variables
Data were collected by reviewing the UMIC electronic databases. Hyperkalemia was defined as serum potassium ≥5.0 mEq/L, and severity ranges were based on those proposed by the European Society of Cardiology (ESC). (17)
Statistical analysis
Qualitative variables were expressed as frequencies and percentages, while continuous quantitative variables were reported as mean and standard deviation (SD) or median and interquartile range (IQR). The chi-square test was used to assess the association between qualitative variables. Student’s t-test was used for differences in normally distributed continuous variables, and the Mann-Whitney U test for nonnormally distributed variables. The level of significance was set at alpha = 0.05.
Ethical considerations
The study was conducted in accordance with the ethical considerations of the World Medical Association’s Declaration of Helsinki. (18) and the project was approved by the Hospital de Clínicas ethics committee.
RESULTS
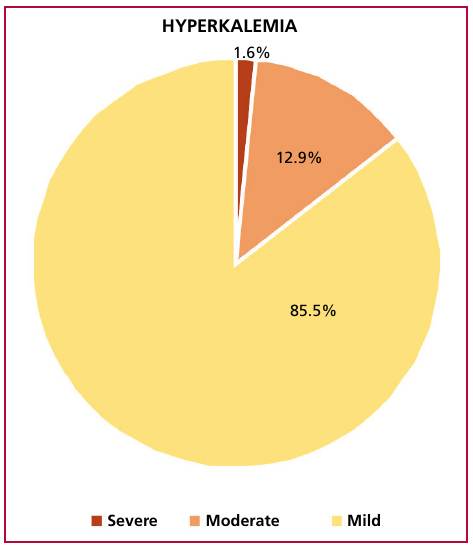
Among a total cohort of 1050 patients with heart failure, 693 meeting the inclusion criteria were included in the study, 69.8 % (478) of whom were women. The median population age was 73 years (IQR 64-81.5) and the prevalence of hyperkalemia was 27% (95% CI 23-30). Mean potassium level was 4.55 ± 0.61 mEq/L. The analysis of subgroups showed that patients with hyperkalemia had a mean potassium level of 5.28 mEq/L vs. 4.29 mEq/L in the rest of patients. Regarding disease severity, the most common presentation was mild (85.5%), compared with 12.9% moderate and only 1.6% severe (Figure 1).
Fig. 1
Degree of hyperkalemia. Most patients presented mild hyperkalemia, while only a very limited number of cases were severe
The association between hyperkalemia and relevant clinical variables is presented in Table 1. The prevalence was 28.2% (135/478) for females and 23.7% (51/215) for males, with no significant difference (p = 0.214). Neither significant difference was observed between patients with and without hyperkalemia in terms of age (p = 0.654) or presence of diabetes (p = 0.324).
Table 1
Prevalence of hyperkalemia and clinical variables
| Clinical variable | All | Hyperkalemia YES | Hyperkalemia NO | p |
|---|---|---|---|---|
| (n=693) | (n=186) | (n=507) | ||
| Age, years, mean ± SD | 75 (± 13.02) | 72.47 (± 12.54) | 71.48 (± 13.20) | 0.654 |
| Diabetes Mellitus, n (%) | 225 (32.5) | 55 (29.6) | 170 (33.5) | 0.324 |
| Hypertension, n (%) | 596 (86.0) | 161 (86.6) | 435 (85.8) | 0.798 |
| CKD, n (%) | 280 (40.4) | 88 (47.3) | 192 (37.9) | 0.026 |
| FC Dyspnea, n (%) | ||||
| 0 | 3 (0.4) | ---- | 3 (0.6) | ---- |
| 1 | 217 (31.3) | 60 (32.3) | 157 (31.0) | 0.816 |
| 2 | 314 (45.3) | 87 (46.8) | 227 (44.9) | 0.702 |
| 3 | 147 (21.2) | 38 (20.4) | 109 (21.5) | 0.841 |
| 4 | 11 (1.6) | 1 (0.5) | 10 (1.9) | 0.319 |
| Ischemic heart disease, n (%) | 397 (57.3) | 114 (61.3) | 283 (55.9) | 0.206 |
CKD: chronic kidney disease; FC: functional class; SD: standard deviation
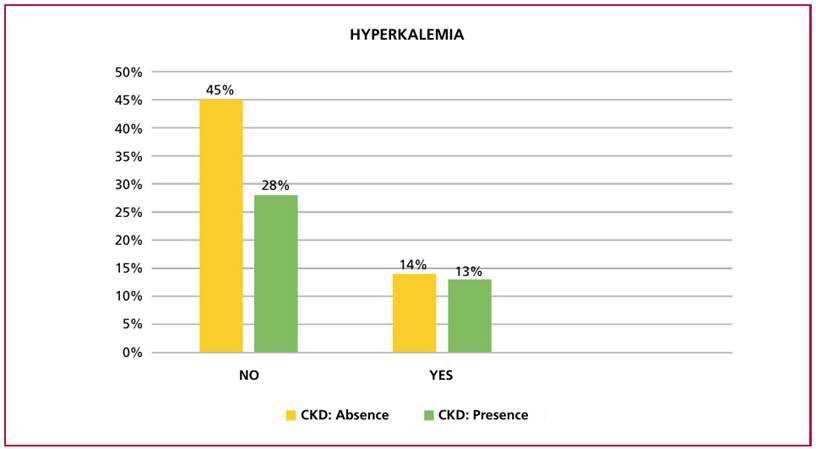
Notably, there was a statistically significant association between hyperkalemia and the presence of CKD (OR 1.469, 95% CI 1.046-2.062, p = 0.026) (Figure 2).
Fig. 2
Hyperkalemia and CKD. The relative frequency of hyperkalemia is higher, though not exclusive, in patients with chronic kidney disease (CKD). The absence of hyperkalemia is associated more closely with absence of CKD.
Regarding renal functional parameters, there was a clear association with reduced glomerular filtration rate and increased azotemia (Table 2).
Table 2
Presence of hyperkalemia and other parameters studied
| All | Hyp erkalemia YES | Hyp erkalemia NO | p | |
|---|---|---|---|---|
| (n=693) | (n=186) | (n=507) | ||
| Creatinine (mg/dL)* | 1.1 (0.9 - 1.4) | 1.2 (0.9 - 1.5) | 1.1 (0.9 - 1.4) | 0 .5 23 |
| eGFR CKD/EPI** | 67.0 ± 1.4 | 62.7 ± 1.7 | 68.6 ± 1.2 | 0 .0 07 |
| Azotemia g/L* | 45.5 (34.3 - 62.0) | 50.0 (38.0 - 67.0) | 44.0 (33.0 - 60.0) | 0 .0 03 |
*values expressed as median (IQR); **values expressed as mean ± SD eGFR CKD/EPI: glomerular filtration rate according to the CKD/EPI formula
Table 3 presents the relationship between hyperkalemia and stages of glomerular filtration rate. A strong association with stage 3B is notable.
The relationship between the presence of hyperkalemia and standard therapy for HF is detailed in Table 4. No statistically significant difference was observed in any of the cases.
DISCUSSION
Hyperkalemia in patients with HFrEF is common and is associated with increased morbidity and mortality. (19, 20) This first study in the UMIC cohort (Montevideo) found a prevalence of 27%, a figure higher than the 8-25% range reported internationally. (21, 22). Most cases were mild and were significantly associated with stage 3B CKD, a stage at which potassium excretion is significantly impaired. (23)
No significant association was found in stages 4-5 CKD. This could be explained by the small sample size in this subgroup, or by marked clinical caution and therapeutic inertia, characterized by low prescription of disease-modifying drugs (DMDs) due to the risk of severe hyperkalemia. (9, 16, 24) These findings underscore the clinical dilemma of balancing the benefits of DMDs against the risk of complications related to impaired potassium homeostasis in patients with advanced kidney disease, a group frequently excluded from clinical trials. (24)
Regarding treatment, the lack of an association between the use of ACEI/ARB II or mineralocorticoid antagonists and hyperkalemia differs from international reports describing a significantly higher incidence of hyperkalemia events in patients on triple therapy. (25) This finding may be attributed to the homogeneity of the sample due to the high local prescription rate, but it also suggests the success of optimized treatment regimens. The concomitant use of SGLT2i s likely exerts a compensatory diuretic effect that neutralizes the risk of elevated potassium. (26) Therefore, the risk associated with these drugs appears manageable under close monitoring in specialized units.
Among the study’s strengths are the availability of a large, well-characterized cohort with standardized definitions according to international guidelines, allowing for precise risk stratification by CKD stage. As limitations, the retrospective observational design and the setting in a specialized unit may introduce selection and referral biases. These factors, along with therapeutic adjustment based on the risk of low baseline potassium levels, should be considered when generalizing the results.
Table 3
Presentation of the relationship between hyperkalemia and glomerular filtration rate stages
| Stage | All | Hyp erkalemia YES | Hyp erkalemia NO | p |
|---|---|---|---|---|
| (n =693) | (n=186) | (n=507) | ||
| 1, n (%) | 133 (19.3) | 27 (14.8) | 106 (21.0) | 0 .0 71 |
| 2, n (%) | 262 (38.1) | 64 (35,0) | 198 (39.2) | 0 .2 87 |
| 3 A, n (%) | 152 (22.1) | 45 (24.6) | 107 (21.2) | 0 .4 58 |
| 3 B, n (%) | 94 (13.7) | 37 (20.2) | 57 (11.3) | 0 .0 05 |
| 4, n (%) | 34 (4.9) | 8 (4.4) | 26 (5.1) | 0 .7 96 |
| 5, n (%) | 13 (1.9) | 2 (1.1) | 11 (2.2) | 0 .5 28 |
Table 4
Occurrence of hyperkalemia and standard HF therapy
| Stage | All | Hyp erkalemia YES | Hyp erkalemia NO | p |
|---|---|---|---|---|
| (n =693) | (n=186) | (n=507) | ||
| ACEI - ARB II* , n (%) | 585 (84.4) | 156 (83,9) | 429 (84,6) | 0 .9 66 |
| Beta-blockers, n (%) | 621 (89,6) | 172 (92,5) | 449 (88,6) | 0 .1 35 |
| Loop diuretics, n (%) | 429 (61,9) | 109 (58,6) | 320 (63,1) | 0 .2 78 |
| Thiazides, n (%) | 26 (3,8) | 4 (2,2) | 22 (4,3) | 0 .1 83 |
| Spironolactone, n (%) | 184 (26,6) | 52 (28,0) | 132 (26,0) | 0 .6 12 |
| ARNI, n (%) | 19 (2,7) | 5 (2,7) | 14 (2,8) | 0 .9 58 |
| Statins, n (%) | 408 (58,9) | 115 (61,8) | 293 (57,8) | 0 .3 39 |
| Antiplatelet agents, n (%) | 292 (42,1) | 86 (46,2) | 206 (40,6) | 0 .1 85 |
| SGLT2i n (%) | 26 (3,8) | 9 (4,8) | 17 (3,4) | 0 .3 62 |
ACEI: angiotensin-converting enzyme inhibitors ARB II: angiotensin II receptor blockers; ARNI: angiotensin receptor neprilysin inhibitors; SGLT2i: sodium-glucose cotransporter 2 inhibitors
* 577 ACEI patients, 8 ARA II patients.
CONCLUSIONS
The prevalence of hyperkalemia in patients with HFrEF in our cohort is high, with the majority of cases being mild. Hyperkalemia is primarily associated with the presence of CKD, especially in 3B stage. The absence of a significant association between hyperkalemia and the use of DMDs highlights the importance of maintaining disease-modifying therapy, aimed at reducing morbidity and mortality in this patient group.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web).
Funding
Personal resources.