Durabilidad de prótesis valvulares aórticas biológicas: deterioro estructural e incidencia de eventos en el seguimiento alejado
Rev Argent Cardiol 2024;92:271-277. http://dx.doi.org/10.7775/rac.v92.i4.20794
Received: 03/11/2024 Accepted: 06/03/2024
Correspondence: Daniel Navia. Instituto Cardiovascular, ICBA. donavia@icba.com.ar
MTSAC Miembro Titular de la Sociedad Argentina de Cardiología

INTRODUCTION
Severe aortic stenosis is the most common primary valve disease, with an increased prevalence in the last few decades due to a higher life expectancy for general population. (1) More than 400 000 aortic valve replacements (AVR) are performed annually worldwide, with important social and economic consequences. It is estimated that in 2050 this procedure will be performed in more than 850 000 patients. (2)
In recent years, there has been a shift in the choice of the prosthesis type, with priority towards the use of biological valves over mechanical valves, even in patients younger than 60. Nowadays, it is estimated that bioprostheses are used in 80% of aortic valve replacements worldwide. (3) This is a consequence of a significant improvement in valve durability and the desire to avoid definitive anticoagulation. (4) There have been improvements in the hemodynamic profile of the prostheses, and changes in the methods of tissue preservation. Although bioprosthetic valves do not require anticoagulation, their shorter long-term durability represents their main limitation, requiring reoperation during the long-term follow-up. We have the latest generation of valve prostheses, but their durability and the incidence of long-term events still remain to be studied. This study aims to evaluate the long-term performance of bioprosthetic aortic valves in relation to survival, the need for reoperation and the echocardiographic incidence of structural valve deterioration (SVD) in a consecutive group of patients undergoing elective and emergency surgery.
METHODS
Between January 2003 and December 2023, 2635 patients underwent bioprosthetic AVR, either electively or urgently, and were prospectively and consecutively entered into a general database. Patients with coronary artery bypass grafting were included but those with pure aortic regurgitation, diagnosis of valve infection, mitral valve compromise, and thoracic aortic surgery were excluded. Preoperative baseline characteristics and intraoperative variables were analyzed in overall population. In patients without coronary artery disease (n=448), AVR was performed by a minimally invasive technique through an upper hemisternotomy in the third or fourth intercostal space with femoral venous drainage by puncture using the Seldinger technique, guided by intraoperative transesophageal echocardiography (TEE). (5) In the analysis of early postoperative results and long-term follow-up, patients were divided according to age (< or ≥60 years) and prosthesis size (< or ≥23 mm). In-hospital mortality was defined as mortality during hospitalization or in the 30-day postoperative period. In-hospital mortality, deep sternal infection (mediastinitis), postoperative acute myocardial infarction (AMI) and postoperative stroke (central neurological deficit lasting more than 72 hours, regardless its confirmation by computed tomography), reoperation for bleeding, renal failure requiring dialysis, and the need for a permanent pacemaker were analyzed. Early postoperative data were obtained from medical records during hospitalization. At long-term follow-up, survival and the presence of events were assessed. The follow-up was carried out by direct communication with patients, their family members, and the general practitioner, as well as by medical records review. The presence of a new stroke and signs of congestive heart failure (CHF) due to prosthetic valve dysfunction were considered reasons for reoperation, and the need for valve replacement was considered to assess the reoperation-free period.
Long-term follow-up data were obtained from cardiology office visits, general practitioner’s records, and/or telephone calls. The date of the last visit recorded at follow-up database was defined as evidence of long-term survival according to Kaplan-Meier analysis.
An echocardiographic follow-up was performed. The baseline study was the one conducted within 90 days of surgery, and the long-term follow-up included studies performed 5 and 10 years after surgery. A Phillips Epiq 7 equipment (Philips Medical Systems, Andover, MA) with matrix 5-1 transducer was used. Although many data were obtained from prosthetic function (ejection fraction, outflow tract velocity, effective orifice area, presence of periprosthetic leaks, prosthetic valve regurgitation, and so on), we considered the values of the mean transprosthetic gradient (mTPG) at baseline and at follow-up to be the most representative data of structural valve deterioration (SVD). According to the American Society of Echocardiography (ASE), SVD was defined as possible prosthetic stenosis in the presence of a mean gradient from 20 to 25 mmHg, and as significant prosthetic stenosis in the presence of a mean gradient ≥35 mmHg. (6)
We considered the recommendations of the European Association for Cardiovascular Imaging (EACVI), which considers as possible prosthetic stenosis an increase in mean gradient of 10-19 mmHg and as significant prosthetic stenosis an increase in mean gradient greater than 20 mmHg. (7)
In addition to the long-term survival according to age and the prosthesis size, we analyzed the period free from readmission due to cardiological diseases, the period free from reoperation and the incidence of SVD at long-term follow-up.
This study aimed to evaluate the performance of bioprosthetic valves in relation to long-term survival, the need for readmission and reoperation, and to describe the echocardiographic incidence of SVD according to changes in mTPG at long-term follow-up by age and prosthesis size.
Statistical analysis
Time-to-event analysis was performed according to Kaplan-Meier method for survival, freedom from reoperation and freedom from readmission at 10 years. Differences in time-to-event curves between groups were analyzed by the log-rank test. Patient characteristics were expressed as mean ± standard deviation, median and interquartile range (IQR) or prevalence (in percentage), as appropriate. Differences between groups were analyzed with Student's t test for continuous variables with normal distribution, with the Mann-Whitney U test for continuous variables with non-normal distribution, and the chi-square test for categorical variables. A value of p <0.05 was considered statistically significant.
The statistical software IBM ® SPSS ® Statistics (version 21) was used.
RESULTS
A total of 2635 patients were included in the study. The mean age was 73±3.05 years; 105 patients were younger than 60 years, and 2530 patients were 60 years or older. Of them, 63.4% were male. Combined procedures were carried out in 1135 patients (43%). A minimally invasive approach was performed in 16.6%, and in 73% of the cases the prosthesis size was ≥23 mm. The type of implanted prosthesis was pericardial in 509 patients (19.4%) and non-pericardial in 2126 patients (80.6%). Overall in-hospital mortality was 2.9%; the incidence of stroke was low (0.6%) and the need for permanent pacemaker was 2.8%. (Table 1)
Table 1
Patients’ baseline characteristics
Quantitative variables are expressed as median and interquartile range.
In patients with known coronary artery disease who underwent combined procedures, the mean number of grafts was 2.06±0.6. Although the analysis of perioperative complications was not the purpose of this study, they are shown in Table 2.
Table 2
Early postoperative results
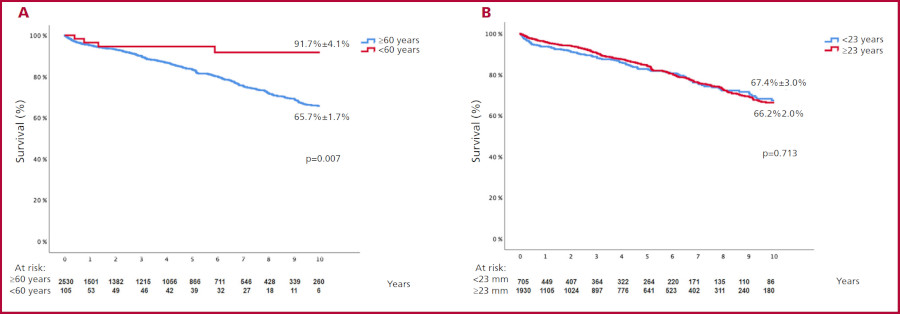
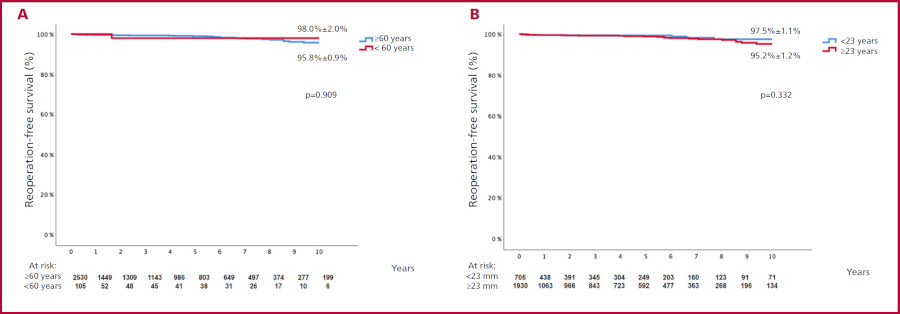
The long-term follow-up was complete in 92% of patients, with a mean of 5.9±3.2 years. Survival at 5 and 10 years according to age was: in patients <60 years 98.3 and 91.7%, vs. in patients ≥60 years 81.7 and 65.7% (p=0.007), respectively. There were no significant differences in the long-term survival according to the prosthesis size: <23 mm: 67.5% vs. ≥23 mm: 66.2% (p=NS). (Figure 1) The 10-year survival free from readmission for cardiac diseases was low, and without significant differences between groups (94.7% vs. 86.1%, p=NS). The 10-year period freedom from reoperation was greater than 95%, with no statistical differences according to age and the implanted prosthesis size. (Figure 2).
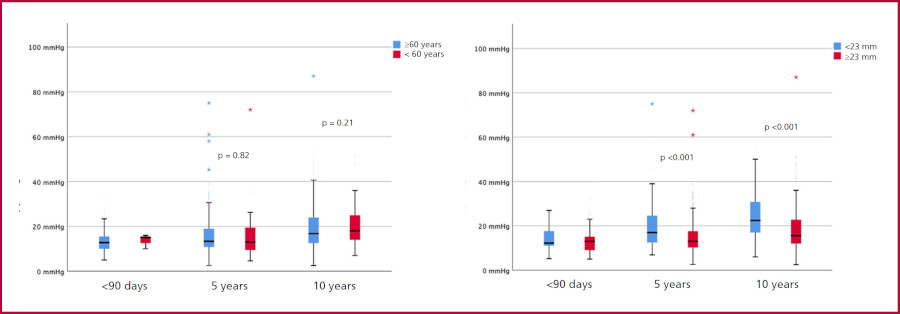
An overall echocardiographic follow-up was performed in 1399 patients (59.7%): at baseline in 845, at 5 years in 473 and at 10 years in 101 patients. The changes in mTPG at 5 and 10 years from baseline were analyzed. This analysis was performed a) according to age: in patients <60 years: 16±3 mmHg, 16±6 mmHg and 19±5 mmHg vs. in patients ≥60 years: 15±5 mmHg, 16±7 mmHg and 18±7 mmHg (p= NS), and b) according to implanted prosthesis size: <23 mm: 17±6 mmHg, 19±7 mmHg and 22±7 mmHg vs. ≥23 mm: 15±5 mmHg, 16±6 mmHg and 18±6 mmHg (p=0.001). (Figure 3)
DISCUSSION
In surgical AVR, bioprosthetic valves are increasingly implanted to the detriment of mechanical valves. (8) Biological tissues are used in most procedures, and currently in percutaneous valve implantations. This tissues have low thrombotic effect, and do not need patient’s permanent anticoagulation. However, bioprostheses have disadvantages related to their limited durability due to SVD.
Age (>70 years) has been a limiting factor for the indication of bioprosthetic valves. Recently, the European Society of Cardiology (ESC) guidelines have recommended biological prostheses in patients over 65 years. (9) In contrast, the American Heart Association/American College of Cardiology (AHA/ACC) guidelines consider biological prostheses in patients over 50 years to be reasonable. (10) In the AUTHEARTVISIT study, Traxler et al. assessed surgical valve replacement in young patients (<50 years) and demonstrated that patients with bioprosthetic valves have a higher incidence of reoperations and a shorter reoperation-free period than the group of patients with mechanical valves. (11) This evolutionary damage depends on many factors (age, prosthesis type and size, etc.). In our setting, we have the latest generation of bovine pericardial valves with improved design to ensure better hemodynamics, and with improvements in tissue preservation processes. An example of this is the INSPIRIS RESILIA Aortic Valve (INSPIRIS; Edwards Lifesciences Corporation, Irvine, CA, USA) which combines a new design with new tissue preservation techniques. A recent study of 689 patients who underwent surgery with this type of prosthesis (66.9±11.6 years of age) experienced a very low incidence of SVD at a 7-year echocardiographic follow-up, which was showed by mTPG values lower than 12 mmHg. (12)
SVD usually presents as leaflet calcification resulting in stenosis, but it may also develop as severe valve regurgitation due to leaflet tearing. Definitions and criteria for classifying SVD have changed over time. Dvir et al. have proposed a set of practical and standardized definitions to clinically and echocardiographically assess SVD at long-term follow-up. (13)
This classification is crucial to define the accurate durability of bioprostheses; it is known that relying on the need for reoperation often underestimates the incidence of SVD, since many patients are considered at high-risk for valve reoperation.
Meta-analyses involving porcine and bovine pericardial valves have shown that SVD usually begins 8 years after surgery with a marked increase 10 years after surgery. (14,15) Although the presence of SVD usually includes increased leaflet thickness, leaflet calcification or tissue tearing with stenosis and/or regurgitation detected by computed tomography, changes in mTPG at long-term follow-up from baseline are the strongest indicator of suspected prosthetic damage, whether moderate or severe. (16) The experience published by several surgical groups describes a low incidence of severe SVD at long-term follow-up without a clear direct relationship with age dichotomized at 65 years. (17,18) However, in young patients (<50 years) the incidence of severe SVD is significantly more frequent. (19) In our series, on 1399 echocardiograms evaluated during a 10-year follow-up, the presence of severe SVD has been low and with no statistical differences according to age. There was a significant statistical difference in the mTPG at 5- and 10-year follow-up according to the prosthesis size, although these values were lower than those considered severe (mTPG in <23 mm = 22 mmHg vs. in ≥23 mm = 18 mmHg).
According to most publications, the incidence of severe patient-prosthesis mismatch is low. Patient-prosthesis mismatch could accelerate the development of early SVD. Currently, surgical techniques to enlarge the aortic annulus are used to adjust the size of the aortic valve prosthesis to the patient’s body surface area. (20,21)
In this study, prosthetic valve sizes ≥23 mm were implanted in 73% of patients considering their body surface area.
Limitations
Our study has several limitations: it was a retrospective and single-center analysis. However, it should be noted that all consecutively included patients represent a good sample of the real-world daily practice.
Despite the long study period, 92% of patients were followed-up. The echocardiographic study at long-term follow-up could only be performed in 59% of patients. Many patients underwent their studies sporadically and in other sites, without a clear follow-up protocol. The long-term follow-up of this study took place during the pandemic period showing a marked negative effect as regards collecting evolutionary data. Despite these limitations, it was possible to analyze a non-negligible sample of 1399 echocardiographic studies performed in 10-year period. Only the changes in mTPG over time were important for analysis, and our experience, in terms of incidence and severity of SVD, coincides with that of most of the different groups worldwide.
CONCLUSION
Patients with bioprosthetic valves had a high long-term survival with significant differences according to age group. The reoperation-free period was high for all patients. Although there were significant mean changes in mTPG in the group of patients with prosthesis size <23 mm at 5- and 10-year follow-up, these differences were less than 10 mmHg from baseline, demonstrating a low incidence of long-term severe SVD. There were no significant differences in the mTPG values according to age.
BIBLIOGRAFIA
1. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al; ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38:2739-91. https://doi.org/10.1093/eurheartj/ehx391
2. Moore M, Chen J, Mallow PJ, Rizzo JA. The direct health-care burden of valvular heart disease: evidence from US national survey data. Clinic Outcomes Res. 2016;8:613-27. https://doi.org/10.2147/CEOR.S112691 .
3. Salaun E, Clavel MA, Rodés-Cabau J, Pibarot P. Bioprosthetic aortic valve durability in the era of transcatheter aortic valve implantation. Heart. 2018;104:1323-32. https://doi.org/10.1136/heartjnl-2017-311582
4. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Fleisher LA, et al, Sundt TM 3rd, Thompson A. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;70:252-89. https://doi.org/10.1016/j.jacc.2017.03.011
5. Shekar PS. Minimal access aortic valve surgery through an upper hemisternotomy approach. Operative Techniques in Thoracic and Cardiovascular Surgery: A Comparative Atlas 2010; 15:321-35. https://doi.org/10.1053/j.optechstcvs.2010.11.001
6. Zoghbi WA, Chambers JB, Dumesnil JG, Foster E, Gottdiener JS, Grayburn PA, et al; American Society of Echocardiography's Guidelines and Standards Committee; Task Force on Prosthetic Valves; American College of Cardiology Cardiovascular Imaging Committee; Cardiac Imaging Committee of the American Heart Association; European Association of Echocardiography; European Society of Cardiology; Japanese Society of Echocardiography; Canadian Society of Echocardiography; American College of Cardiology Foundation; American Heart Association; European Association of Echocardiography; European Society of Cardiology; Japanese Society of Echocardiography; Canadian Society of Echocardiography . Recommendations for evaluation of prosthetic valves with echocardiography and doppler ultrasound: a report From the American Society of Echocardiography's Guidelines and Standards Committee and the Task Force on Prosthetic Valves, developed in conjunction with the American College of Cardiology Cardiovascular Imaging Committee, Cardiac Imaging Committee of the American Heart Association, the European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography and the Canadian Society of Echocardiography, endorsed by the American College of Cardiology Foundation, American Heart Association, European Association of Echocardiography, a registered branch of the European Society of Cardiology, the Japanese Society of Echocardiography, and Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2009;22:975-1014; quiz 1082-4. https://doi.org/10.1016/j.echo.2009.07.013
7. Lancellotti P, Pibarot P, Chambers J, Edvardsen T, Delgado V, Dulgheru R, et al. Recommendations for the imaging assessment of prosthetic heart valves: a report from the European Association of Cardiovascular Imaging endorsed by the Chinese Society of Echocardiography, the Inter-American Society of Echocardiography, and the Brazilian Department of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2016; 17:589-90. https://doi.org/10.1093/ehjci/jew025
8. Isaacs AJ, Shuhaiber J, Salemi A, Isom OW, Sedrakyan A. National trends in utilization and in-hospital outcomes of mechanical versus bioprosthetic aortic valve replacements. J Thorac Cardiovasc Surg. 2015;149:1262-9.e3. https://doi.org/10.1016/j.jtcvs.2015.01.052
9. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al; ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632. https://doi.org/10.1093/eurheartj/ehab395
10. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F, et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e35-e71. https://doi.org/10.1161/CIR.0000000000000932
11. Traxler D, Krotka P, Reichardt B, Copic D, Veraar C, Mildner M, et al. Revisiting aortic valve prosthesis choice in patients younger than 50 years: 10 years results of the AUTHEARTVISIT study. Eur J Cardiothorac Surg. 2024;65: ezad308. https://doi.org/10.1093/ejcts/ezad308
12. Bernard J, Georges G, Hecht S, Pibarot P, Clavel MA, Babaki S, et al. Mid-term clinical and echocardiographic results of the INSPIRIS RESILIA aortic valve: a retrospective comparison to the Magna Ease. Interdiscip Cardiovasc Thorac Surg. 2023;37: ivad117. https://doi.org/10.1093/icvts/ivad117.
13. Dvir D, Bourguignon T, Otto CM, Hahn RT, Rosenhek R, Webb JG, et al; VIVID (Valve in Valve International Data) Investigators. Standardized Definition of Structural Valve Degeneration for Surgical and Transcatheter Bioprosthetic Aortic Valves. Circulation. 2018;137:388-99. https://doi.org/10.1161/CIRCULATIONAHA.117.030729
14. Wang M, Furnary AP, Li HF, Grunkemeier GL. Bioprosthetic Aortic Valve Durability: A Meta-Regression of Published Studies. Ann Thorac Surg. 2017; 104:1080-7. https://doi.org/10.1016/j.athoracsur.2017.02.011
15. Jung YJ, Choi JW, Kang Y, Kim JS, Sohn SH, Hwang HY, et al. Long-term results of a stented bioprosthetic valve in the aortic position: structural valve deterioration and valve haemodynamic deterioration of bovine pericardial and porcine valves. Eur J Cardiothorac Surg. 2023;63: ezac506. https://doi.org/10.1093/ejcts/ezac506
16. Capodanno D, Petronio AS, Prendergast B, Eltchaninoff H, Vahanian A, Modine T, et al. Standardized definitions of structural deterioration and valve failure in assessing long-term durability of transcatheter and surgical aortic bioprosthetic valves: a consensus statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI) endorsed by the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur J Cardiothorac Surg. 2017; 52:408-17 https://doi.org/10.1093/ejcts/ezx244
17. Bourguignon T, Lhommet P, El Khoury R, Candolfi P, Loardi C, Mirza A, et al. Very long-term outcomes of the Carpentier-Edwards Perimount aortic valve in patients aged 50-65 years. Eur J Cardiothorac Surg. 2016; 49:1462-8. https://doi.org/10.1093/ejcts/ezv384
18. Forcillo J, El Hamamsy I, Stevens LM, Badrudin D, Pellerin M, Perrault LP, et al. The perimount valve in the aortic position: twenty-year experience with patients under 60 years old. Ann Thorac Surg. 2014;97:1526-32. https://doi.org/10.1016/j.athoracsur.2014.02.019
19. Piperata A, Fiocco A, Cavicchiolo A, Ponzoni M, Pesce R, Gemelli M, et al. Carpentier-Edwards Magna Ease bioprosthesis: a multicentre clinical experience and 12-year durability. Eur J Cardiothorac Surg. 2022; 61:888-96. https://doi.org/10.1093/ejcts/ezab552
20. Côté N, Pibarot P, Clavel MA. Incidence, risk factors, clinical impact, and management of bioprosthesis structural valve degeneration. Curr Opin Cardiol. 2017; 32:123-9. https://doi.org/10.1097/HCO.0000000000000372
21. Francica A, Benvegnù L, San Biagio L, Tropea I, Luciani GB, Faggian G, et al. Ten-year clinical and echocardiographic follow-up of third-generation biological prostheses in the aortic position. J Thorac Cardiovasc Surg. 2022: S0022-5223(22)01142-4. https://doi.org/10.1016/j.jtcvs.2022.10.023