
Infective endocarditis is still a diagnostic challenge due to its variable clinical presentation. The most common associated microorganisms are Staphylococcus aureus and streptococci of the oral cavity, and, to a lesser extent, Enterococcus faecalis. We report the case of a young patient with infective endocarditis caused by Neisseria gonorrhoeae, a relatively uncommon etiology. (1-3)
A 28-year-old otherwise healthy male, with a history of tobacco use and overweight, presented to a local hospital with a three-week history of fever, abdominal pain, and diarrhea. Internal Medicine reviewed the case and diagnosed the patient with uncomplicated diverticulitis. Of the two blood cultures taken, one resulted positive for N. gonorrhoeae. Antibiotic treatment was therefore initiated with metronidazole, ceftriaxone and doxycycline to cover both sites of infection. The patient denied engaging in risky sexual behaviors and tested negative for sexually transmitted infections. Physical examination revealed a previously unknown grade 3/6 diastolic murmur at the aortic area. Consequently, the patient underwent transthoracic and transesophageal Doppler echocardiography. Both imaging modalities revealed a 9 mm x 4 mm vegetation on the non-coronary cusp of the aortic valve, associated with severe regurgitation (Figures 1 and 2). Additionally, the left ventricle was mildly dilated (measuring 6.2 cm in diastole on transesophageal echo), and a 6.3 mm mobile, pedunculated vegetation was observed on the atrial aspect of the P1-P2 segments of the mitral valve; this mass prolapsed into the ventricle during diastole without causing valvular dysfunction.
Fig. 1
Short-axis view and long-axis view showing vegetation on the noncoronary cusp of the aortic valve.
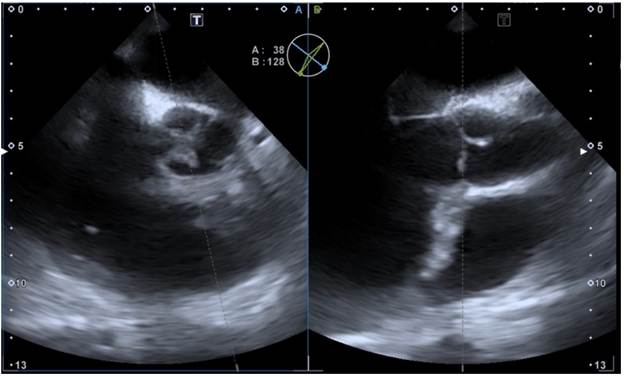
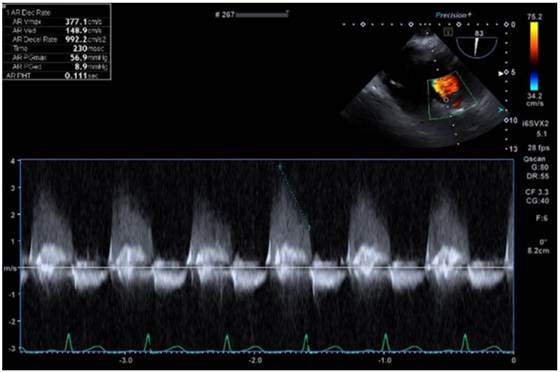
Fig. 2
A severe regurgitant jet was observed in the transgastric view, with a PHT of 0.11 s and a deceleration rate of 992 cm/s at the aortic valve level.
The clinical picture was interpreted as definitive native valve infective endocarditis, caused by Neisseria gonorrhoeae, involving both the aortic valve and mitral valve. There were no signs of septic embolism. The patient was admitted to a general ward and remained haemodynamically stable, with no evidence of arrhythmias on telemetry or abnormalities on the baseline electrocardiogram.
Due to severe acute aortic regurgitation associated with infective endocarditis, surgery was decided once antibiotic therapy for diverticulitis with metronidazole and ceftriaxone had been completed. Aortic valve replacement was performed using a 21 mm mechanical prosthesis, with debridement of an abscess in the mitral-aortic intervalvular fibrosa and placement of an autologous pericardial patch. An atrial septal defect closure was also performed. Intraoperative transoesophageal echocardiogram confirmed adequate prosthetic valve function without associated regurgitation or mismatch. The excised native valve tested positive for N. gonorrhoeae via polymerase chain reaction (PCR). Antibiotic treatment with ceftriaxone was continued, and anticoagulation was indicated due to the mechanical valve.
The patient had a favorable postoperative course and was discharged to complete antibiotic treatment at home for a total of 6 weeks following aortic valve replacement.
N. gonorrhoeae endocarditis is a rare and infrequently reported entity. Clinical suspicion based on compatible physical findings and early echocardiography are essential for diagnosis. (4,5)
Conflicts of interest
None declared.
(See conflicts of interest forms on the website).
Ethical considerations
Not aplicable.