Hipertensión arterial nocturna: análisis según su gravedad
Rev Argent Cardiol 2024;92:263-270. http://dx.doi.org/10.7775/rac.v92.i4.20798
SEE RELATED ARTICLE: Rev Argent Cardiol 2024;92:261-262. http://dx.doi.org/10.7775/rac.v92.i4.20793
Received: 06/03/2024 Accepted: 07/10/2024
Correspondence: Joaquín Perea. E-mail: joacoperea33@gmail.com. Research Department Sanatorio Güemes. Francisco Acuña de Figueroa 1228, 7th Floor, CP 1180AAX, City of Buenos Aires, Argentina.
MTSAC Miembro Titular de la Sociedad Argentina de Cardiología

INTRODUCTION
The global prevalence of atherosclerotic cardiovascular disease continues to rise due to the increase of risk factors such as obesity, unhealthy lifestyles and population aging. (1,2) Hypertension (HTN) is recognized as one of the most significant risk factors, and has a high worldwide prevalence; therefore, it is crucial to make a correct diagnosis and treatment. (3)
Most international guidelines recommend ambulatory blood pressure monitoring (ABPM), which has become essential for the management of patients with HTN, not only for initial diagnosis but also for follow-up and subsequent control. (4,5,6,7) Most studies have shown that 24-hour average blood pressure is a better predictor of cardiovascular events than office blood pressure measurement. (8) In this context we have increasing evidence supporting the superiority of nocturnal hypertension (NHTN) as a predictor of cardiovascular events relative to daytime hypertension, so that ABPM has become essential not only for detection but also for determining its severity. (9,10) There is scarce information about the value of the degree of blood pressure elevation during the nighttime period and its relationship with cardiovascular events and, moreover, from what value of nighttime blood pressure the risk of cardiovascular events begins to increase.
The aim of this study was to find out whether the presence of NHTN and its severity levels are associated with the incidence of cardiovascular adverse events during follow-up.
METHODS
Study design
A retrospective cohort study was conducted including patients who underwent 24-hour blood pressure monitoring for diagnostic confirmation of HTN, or for prognostic purposes, in hypertensive subjects, in a hospital of the Autonomous City of Buenos Aires, Argentina, from March 2017 to December 2022. The composite of adverse cardiovascular events, the so-called major adverse cardiovascular events (MACE) which include cardiovascular death, nonfatal infarction and nonfatal stroke; and hospitalization or visit to the emergency department for heart failure (defined by Framingham criteria), was considered as primary endpoint. Each component of the primary endpoint, in addition to hospitalization for hypertensive urgency/emergency, were considered secondary endpoints.
Study population and definitions
We created our own database, including patients over 18 years of age who underwent pressure monitoring in the Cardiology department.
The variables included in the registry were: a) personal data, gender, age, weight in kg, body mass index (BMI) expressed in kg/m2 (DuBois formula), medical history and classical cardiovascular risk factors; b) from the pressure monitoring data: study date, percentage of successful readings, 24-h averages, daytime and nighttime averages, pulse pressure, nocturnal pattern of blood pressure behavior (dipper, non-dipper, inverted dipper, or hyper dipper); c) laboratory data: creatinine value prior to the study, creatinine clearance value according to the Cockroft-Gault formula, and values at follow-up; d) echocardiographic data: atrial size, septal thickness, posterior wall thickness, left ventricular ejection fraction (LVEF) by Simpson's method; e) antihypertensive treatment with specification of drugs used, use of statins and aspirin.
Patients with technically unsatisfactory studies, duplicate pressure monitoring reports (the first record was included) and those in whom follow-up data could not be obtained were excluded. Follow-up was performed through the institution's electronic medical record.
Nocturnal HTN was defined according to the criteria of the American Heart Association (AHA) taking as reference a blood pressure value ≥120/70 mmHg during the passive/nighttime period, and a value ≥135/85 mmHg in the active/daytime period, both referred in the follow-up chart. (11) We classified NHTN into four severity strata according to nighttime systolic blood pressure: 83-119 mmHg (normal blood pressure), 120-139 mmHg, 140-159 mmHg and 160-220 mmHg.
Procedures
MEDITECH® pressure gauges (model ABPM 05) were used, with oscillometric method and ±3 mmHg accuracy/ 2 % of the measured value according to the manufacturer's technical specifications. They were programmed to take measurements every 15 minutes during the active period and every 30 minutes during the passive period, for 24-hour intervals. Data collection analysis and reporting software was provided by the manufacturer. Follow-up was performed by a group of 4 investigators by consulting the institutional electronic medical record; in cases where the data were incomplete or absent, contact and follow-up were made by telephone and closed-ended questions, for a maximum period of 48 months after the index pressure monitoring.
Statistical analysis
Statistical analyses were performed with R Studio, version 1.4.1106 (The R Foundation for Statistical Computing, Vienna, Austria). Continuous variables are expressed as mean and standard deviation (SD) or median and interquartile range (IQR), according to their distribution. Qualitative variables are expressed as absolute and relative frequencies. Qualitative variables were compared using the chi-square test or Fisher's exact test, while continuous variables with parametric and nonparametric distribution were compared using Student's t test and the Mann Whitney U test, respectively. Multiple imputation of the database was performed for the treatment of missing data, which was carried out through the random forest method since most of the variables imputed were categorical. (12) Bivariate and multivariate analyses were performed to identify factors associated with cardiovascular events. Cox regression models were used to search for predictors of events in the long-term follow-up. All variables that in the bivariate analysis presented a p value <0.20 or that were considered clinically important in relation to the response variable were included in the multivariate model. Nested models were compared and chosen according to Akaike's information criterion, ANOVA and concordance index. Kaplan Meier curves and the log-rank test were performed for variables associated with events at follow-up. The association between predictors and the incidence of events was expressed as Hazard Ratio with its 95% confidence interval (95% CI). All tests were two-tailed and statistical significance was established at p<0.05.
RESULTS
Baseline population characteristics
Out of a total of 1060 initial subjects, 79 cases were excluded from the analysis (60 did not meet the definition of HTN and 19 did not present follow-up). A total of 981 patients remained as the study population. Fifty-three percent were male, and mean age was 59.8±14.2 years. The baseline characteristics of the population stratified according to nighttime systolic blood pressure are shown in Table 1. Sixty four percent of the subjects (n=624) had NHTN. This group had higher BMI, greater prevalence of male gender, diabetes (DM), and as expected, higher daytime systolic and diastolic blood pressure. In the stratified analysis according to the severity of NHTN, we found a positive gradient with respect to cardiovascular risk factors, that is, the higher the degree of nighttime blood pressure, the higher the BMI and the greater the prevalence of DM, sedentary lifestyle and dyslipidemia. Those with higher nighttime blood pressure values had a more frequent history of atrial fibrillation, obstructive sleep apnea-hypopnea syndrome (OSAHS) and echocardiographic repercussion. Patients with NHTN had a lower use of antihypertensive drugs (76 % vs. 86 %, p<0.001). In this group, the most commonly used antihypertensive drugs were angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers.
Table 1
Baseline characteristics of the population stratified according to nocturnal systolic blood pressure.
ACEI: angiotensin-converting enzyme inhibitors; ACS: acute coronary syndrome; AF: atrial fibrillation; ARBs: angiotensin II receptor blockers; BMI: body mass index; CrCl: creatinine clearance; CHF: Chronic heart failure; CV: cardiovascular; DBP: Diastolic blood pressure; HTN: hypertension; IQR: interquartile range; IVS: interventricular septum; LVEF: left ventricular ejection fraction; MACE: major adverse cardiovascular events; OSAHS: obstructive sleep apnea and hypopnea syndrome; PP: pulse pressure; SBP: systolic blood pressure; SD: standard deviation;
Events by group
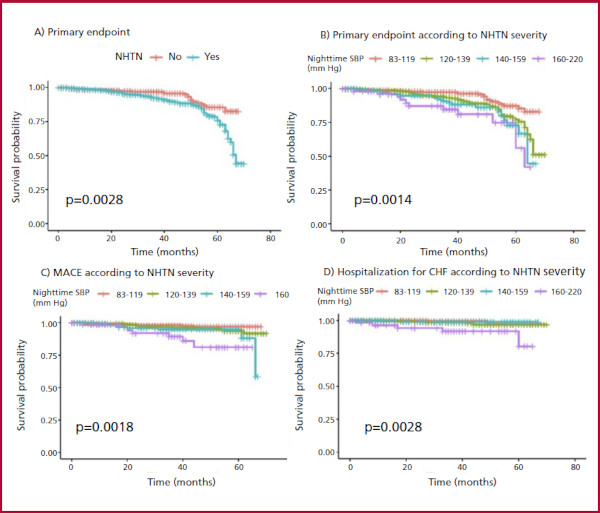
At a median follow-up of 40 (IQR 26-54) months, the main endpoint was present in 130 subjects corresponding to 13.2 % of the total sample, 105 (15.3 %) in the group with NHTN and 25 (8.3 %) in the group without NHTN (p=0.003). In the stratified analysis according to the degree of HTN we found differences between groups in the incidence of: a) the primary endpoint: from 7.6 % between 83-119 mmHg to 24.2 % between 160-220 mmHg (p=0.001); b) MACE: from 2.2 % between 83-119 mmHg to 11.3 % between 160-220 mmHg (p=0.007); c) hospitalization for heart failure: from 1.1 % between 83-119 mmHg to 8.1 % between 160-220 mmHg (p=0.002), and d) hospitalization for hypertensive crisis: from 2.5 % between 83-119 mmHg to 4.8 % between 160-220 mmHg, (p=0.007). Regarding cardiovascular death, although the proportion was higher in the NHTN group, there were no statistically significant differences: from 2.2 % between 83-119 mmHg to 8.1 % between 160-220 mmHg (p=0.102). The probability of event-free survival according to the presence of NHTN, and of the primary endpoint, MACE and hospitalization for heart failure according to the severity of NHTN is shown in Figure 1.
Multivariate analysis: independent predictors of cardiovascular events.
We excluded from the multivariate analysis DM, BMI, OSAHS variables and HTN patterns because they presented a p value >0.20 in the bivariate analysis (Table 2). The remaining variables were evaluated in multivariate analysis with the Cox proportional hazards model. Two regression models were fitted and compared with each other. Model 1 included the NHTN strata, age, smoking, left ventricular hypertrophy, and daytime HTN; and model 2 the same variables except for daytime HTN. The latter model showed the best fit (Table 3), including the severity of NHTN variable as an independent predictor of cardiovascular events, with HR (95% CI) 1.30 (0.65 - 2.58), 2.25 (1.02 - 4.94) and 4.18 (1.60 -10.8) for 120-139, 140-159 and 160-220 mmHg strata, respectively. The NHTN behaved as an independent predictor of cardiovascular events (HR 3.60 95% CI 1.12-11.5 p=0.033). Age and presence of left ventricular hypertrophy variables in the echocardiogram also behaved as independent predictors, with HR (95% CI) 1.04 (1.01-1.06) and 2.35 (1.32-4.20), respectively. When adjusted for the presence of daytime HTN, the severity of NHTN remained as an independent predictor of events, so due to the principle of parsimony it was eliminated from the final model. All the adjusted models complied with the proportional hazards assumptions
Table 2
Bivariate analysis.
Table 3
Multivariate analysis
DISCUSSION
The main finding of our study is the high prevalence of NHTN and its association with cardiovascular outcomes at the long-term follow-up. We observed that this risk begins in the first severity stratum (120-139 mm Hg) and increases exponentially through each stratum, with the highest risk in the highest severity one (160-220 mm Hg). The severity of NHTN behaved as an independent predictor of adverse cardiovascular outcomes, even in the presence of the daytime HTN variable. Age and left ventricular hypertrophy variables in the echocardiogram were also factors associated with poor outcome.
Hypertension is the main modifiable risk factor, and it is possible that the prevalence of the NHTN phenotype is underestimated because its diagnosis depends on the request for 24-h pressure monitoring. (13) In our cohort, this prevalence was 69% and we were able to observe that these patients had a greater number of cardiovascular comorbidities and less antihypertensive treatment. In their work, also carried out in Argentina, Salazar et al (14) found a NHTN prevalence of 61%. Individuals with NHTN had greater history of previous cardiovascular disease (4.2% vs. 1.5%, p= 0.007). These authors found no differences in terms of classical cardiovascular risk factors or in relation to antihypertensive treatment. In another study by Yao Du et al. (15) the reverse dipper or riser pattern was associated with a greater number of comorbidities, including renal dysfunction, overweight and diabetes. In addition to this, they were able to determine that those patients with NHTN presented a 77% higher risk (HR 1.77, 95% CI 1.25-2.50) compared with those without this condition.
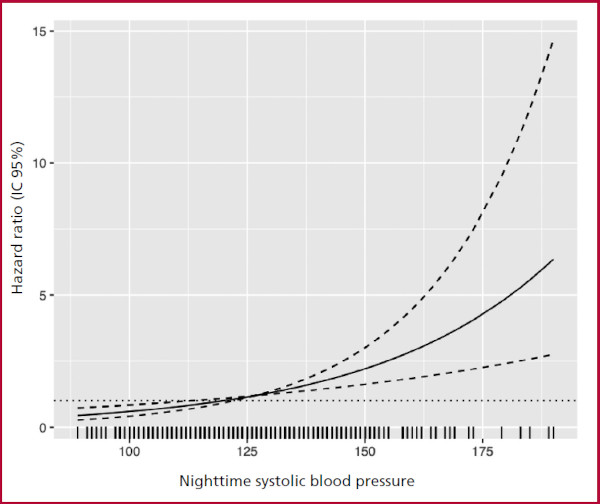
Very few previous studies have studied NHTN according to its severity. (16) We were able to prove that the higher the level of nighttime blood pressure, the higher the risk of cardiovascular events. In addition, we were able to determine that this risk begins to increase very early and close to the reference value by which NHTN is defined (127 mmHg) (Figure 2). This is important, since it not only determines a goal to be achieved by antihypertensive treatment, but also reinforces the notion that nighttime blood pressure measurements carry valuable prognostic information.
Fig. 2
Continuous association between nighttime systolic blood pressure and risk of cardiovascular events. Solid line represents the Hazard Ratio. Dashed lines represent the 95% confidence inter vals. We can observe that the risk starts to increase from 127 mmHg
Hypertension is an important and very frequent comorbidity in patients with a history of heart failure, especially in those with preserved left ventricular ejection fraction. From previous studies we know that more than 50% of patients with heart failure suffer from HTN. (17,18) In their study, Huang et al. in a cohort of patients with a previous diagnosis of heart failure with preserved ejection fraction showed prevalence of HTN in 77% of patients, 40% of which had NHTN. (19) These authors verified that the presence of NHTN is independently associated with rehospitalization for heart failure in the long-term follow-up. In another interesting study carried out by Kidawara et al (20) in patients with diabetes and without previous heart failure, the presence of NHTN behaved as an independent predictor of the progression of left ventricular diastolic dysfunction. In our cohort, as part of an exploratory analysis, we were able to observe a tendency to greater hospitalization for heart failure associated with the presence of NHTN, and that this risk is related to the severity of NHTN.
Our study has some limitations: first and foremost, the retrospective design, which implies biases. Although multivariate regression analysis was performed, we cannot completely rule out the possibility that variables may have altered our results. Secondly, this was a single-center study; however, it was a heterogeneous population with characteristics similar to those of previous studies. Thirdly, as this is a relatively healthy population, we believe that a larger sample size accompanied by a longer follow-up would allow us to determine with greater accuracy the impact of NHTN on cardiovascular events.
In conclusion, in this cohort of patients with HTN the NHTN phenotype and its severity were associated with adverse cardiovascular outcomes at the long-term follow-up.
REFERENCES
2. Goldsborough E 3rd, Osuji N, Blaha MJ. Assessment of Cardiovascular Disease Risk: A 2022 Update. Endocrinol Metab Clin North Am. 2022 ;51:483-509. doi: 10.1016/j.ecl.2022.02.005
3. Fuchs FD, Whelton PK. High blood pressure and cardiovascular disease. Hypertenion. 2020;75:285-92. . https://doi.org/10.1161/HYPERTENSIONAHA.119.14240
4. Leung AA, Nerenberg K, Daskalopoulou SS, McBrien K, Zarnke KB, Dasgupta K, et al; CHEP Guidelines Task Force. Hypertension Canada's 2016 Canadian Hypertension Education Program guidelines for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension. Can J Cardiol 2016;32:569-88. https://doi.org/10.1016/j.cjca.2016.02.066
5. Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/ NMA/PCNA guideline for prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018;71(19):e127-e248. https://doi.org/10.1016/j.jacc.2017.11.006
7. Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al; ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J 2018;39:3021-104. https://doi.org/10.1093/eurheartj/ehy339
8. Dolan E, Stanton A, Thijs L, Hinedi K, Atkins N, McClory S, et al. Superiority of ambula- tory over clinic blood pressure measurement in predicting mortality: the Dublin outcome study. Hypertension 2005;46:156-61. https://doi.org/10.1161/01.HYP.0000170138.56903.7a
9. Sega R, Facchetti R, Bombelli M, Cesana G, Corrao G, Grassi G, et al. Prognostic value of ambulatory and home blood pressures compared with office blood pressure in the general population: follow- up results from the Pressioni Arteriose Monitorate e Loro Associazioni (PAMELA) study. Circulation 2005;111:1777-83. https://doi.org/10.1161/01.CIR.0000160923.04524.5B
10. Hansen TW, Jeppesen J, Rasmussen S, Ibsen H, Torp-Pedersen C. Ambulatory blood pressure and mortality: a population- based study. Hypertension 2005;45:499-504. https://doi.org/10.1161/01.HYP.0000160402.39597.3b
11. Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020 ;75:1334-57. https://doi.org/10.1161/HYPERTENSIONAHA.120.15026
12. Tang F, Ishwaran H. Random Forest Missing Data Algorithms. Stat Anal Data Min 2017;10:363-77. https://doi.org/10.1002/sam.11348
13. Kreutz R, Brunström M, Burnier M, Grassi G, Januszewicz A, Muiesan ML. et añ. European Society of Hypertension clinical practice guidelines for the management of arterial hypertension. Eur Intern Med 2024;126:1-15. https://doi.org/10.1016/j.ejim.2024.05.033
14. Salazar MR, Espeche WG, Balbin E, Leiva Sisnieguez CE, Minetto J, Leiva Sisnieguez BC, et al. Prevalence of isolated nocturnal hypertension according to 2018 European Society of Cardiology and European Society of Hypertension office blood pressure categories. J Hypertens 2020;38:434-40. https://doi.org/10.1097/HJH.0000000000002278
15. Du Y, Zhu B, Liu Y, Zhou W, Du Z, Yang W, et al. Association between nocturnal blood pressure phenotype and adverse cardiovascular prognosis in patients with coronary heart disease and hypertension. J Clin Hypertens 2024;26:405-15. https://doi.org/10.1111/jch.14790
16. Yang W, Y, Melgarejo JD, Thijs L, Zhang ZY, Boggia J, Wei FF, et al. Association of Office and Ambulatory Blood Pressure With Mortality and Cardiovascular Outcomes. JAMA 2019:332:409-20. https://doi.org/10.1001/jama.2019.9811
17. Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med 2006;355:260-9. https://doi.org/10.1056/NEJMoa051530
18. Yancy CW, Lopatin M, Stevenson LW, De Marco T, Fonarow GC; ADHERE Scientific Advisory Committee and Investigators. Clinical presentation, management, and in-hospital outcomes of pati- ents admitted with acute decompensated heart failure with preserved systolic function: a report from the Acute Decompensated Heart Failure National Registry (ADHERE) Database. J Am Coll Cardiol 2006;47:76-84.
19. Huang G, Liu XH, Zhang Y, Zhu YX, He Y, Wang TB, et al. Nocturnal hypertension and riser pattern are associated with heart failure rehospitalization in patients with heart failure with preserved ejection fraction. J Geriatr Cardiol 2023;20:448-58. https://doi.org/10.26599/1671-5411.2023.06.003
20. Kidawara Y, Kadoya M, Igeta M, Morimoto A, Miyoshi A, Kakutani-Hatayama M,et al. Nocturnal Hypertension and Left Ventricular Diastolic Dysfunction in Patients With Diabetes With the Absence of Heart Failure: Prospective Cohort HSCAA Study Hypertension. 2024;81:172-82. https://doi.org/10.1161/HYPERTENSIONAHA.123.21304