
Acute myocardial infarction in children is rare and may be associated with various etiologies, including congenital coronary anomalies, prothrombotic states, and sequelae of Kawasaki disease, the leading cause of acquired heart disease in children.
We present the case of a four-year-old male patient with a history of Kawasaki disease two years prior, without documented structured follow-up. He was admitted with symptoms that had been present for four hours, characterized by vomiting, mucocutaneous pallor, perioral cyanosis, and transient loss of consciousness. On admission, he was hemodynamically stable, with a blood pressure of 90/59 mmHg and a heart rate of 70 bpm.
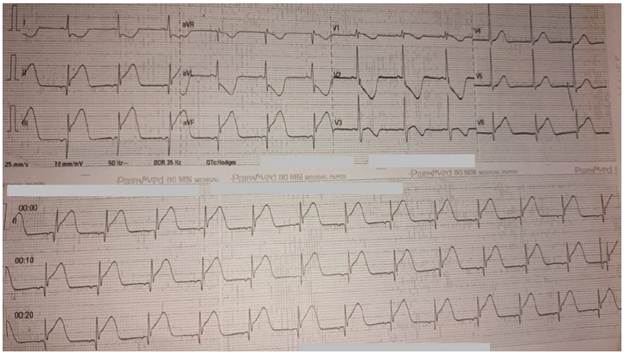
The 12-lead electrocardiogram showed ST-segment elevation in leads II, III, and aVF, with ST-depression in the anterior leads, consistent with acute inferior myocardial infarction (Figure 1). Laboratory results showed C-reactive protein level of 0.14 mg/dL, white blood cell count of 16 770/µL with neutrophilia, hemoglobin 12.1 g/dL, platelets 570 000/µL, creatinine 0.43 mg/dL, and electrolytes within normal ranges. Total creatine kinase was 228 U/L and high-sensitivity troponin I was 0.94 ng/mL, with markedly elevated quantitative troponin level (28 336.7 pg/mL), confirming significant myocardial necrosis.
Fig. 1
Twelve-lead electrocardiogram showing ST-segment elevation in leads II, III, and aVF, with reciprocal changes in the anterior precordial leads, consistent with acute inferior myocardial infarction.
The initial echocardiogram showed preserved biventricular function and mild dilation of the proximal segment of the left coronary artery. Given the suspicion of coronary artery involvement and the limitations of the echocardiographic study in characterizing the distal anatomy, cardiac catheterization was performed at a tertiary care center.
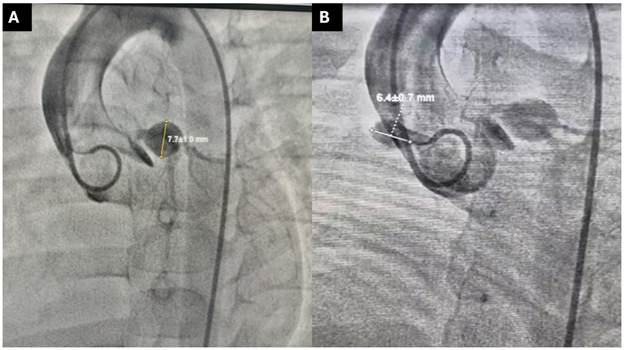
The hemodynamic study revealed a giant aneurysm of the left coronary artery located distal to the trunk and involving the origin of the left anterior descending and circumflex coronary arteries, as well as a proximal aneurysm of the right coronary artery with total occlusion and distal perfusion through collateral circulation (Figure 2). Ventriculography showed inferior wall hypokinesis with preserved global function.
Fig. 2
Coronary angiography (A) Left coronary artery, with a giant aneurysm located distal to the trunk, involving the origin of the anterior descending and circumflex arteries. (B) Right coronary artery, with a proximal aneurysm with total occlusion and distal perfusion via collateral circulation.
Given the anatomical complexity, multivessel involvement, and location of the lesions, it was determined that the risk of percutaneous intervention outweighed the potential benefit; (1,2) therefore, medical management with dual antiplatelet therapy and close follow-up by pediatric cardiology was decided upon. The patient progressed without recurrence of ischemic symptoms.
The clinical presentation of myocardial infarction in children is often atypical, making timely recognition difficult. Unlike in adults, children rarely present with typical chest pain; instead, nonspecific manifestations such as vomiting, pallor, irritability, or altered consciousness predominate. In this context, the integration of electrocardiographic findings consistent with ST-segment elevation and a significant elevation of biomarkers of myocardial necrosis, such as troponin, is essential for establishing the diagnosis. (3,4)
Cardiac catheterization is essential in the evaluation of these patients, as it allows for a precise anatomical characterization of the coronary anatomy, including the identification of aneurysms, occlusions, bifurcation involvement, and the development of collateral circulation. (5) In the case presented, this information was decisive for therapeutic decision-making, as it revealed a complex anatomy with multivessel involvement that limited intervention options.
The management of coronary aneurysms associated with Kawasaki disease depends on their size, location, and the presence of thrombotic or ischemic complications. In patients with giant aneurysms and diffuse involvement, percutaneous intervention can be technically challenging and associated with a higher risk of complications, such as distal embolization, reocclusion, or difficulty in properly implanting devices. Similarly, surgical revascularization is not always feasible, especially in small patients or those with complex anatomy. (6)
In this context, medical treatment with antiplatelet therapy, as initiated in this case, represents a reasonable strategy aimed at reducing the risk of thrombotic events and stabilizing the disease. This approach requires close long-term follow-up, given the persistent risk of cardiovascular complications.
Finally, this case emphasizes the importance of structured follow-up in patients with a history of Kawasaki disease, especially in those with coronary involvement. Regular evaluation allows for the timely detection of vascular abnormalities and appropriate long-term risk stratification. (6) It also highlights the need to consider acute coronary syndrome within the differential diagnosis in pediatric patients with nonspecific symptoms and relevant history, as well as the value of cardiac catheterization in comprehensive evaluation and individualized therapeutic decisionmaking.
Conflicts of interest
None declared.
(See conflicts of interest forms on the website).
Ethical considerations
Not aplicable.