
INTRODUCTION
Acute heart failure (AHF) is associated with high rates of morbidity and mortality and exerts a growing negative impact on public health systems worldwide. (1-3). In this context, AHF is the leading cause of unplanned hospitalizations in patients over 65 years of age, (4) with a threefold increase in hospitalization rates over the past decades due to various factors such as population aging, improved survival following acute myocardial infarction, and delays in the timely diagnosis and treatment of this condition. (5)
Furthermore, patients discharged from a healthcare facility following an episode of AHF frequently have high rehospitalization rates, leading to poorer prognosis. (6) Therefore, the early identification of patients at high risk of readmission prior to hospital discharge is essential, especially in the elderly population with multiple comorbidities.
Volume overload and congestion are present in 95% of patients with acute AHF. (7) Despite treatment with diuretics, a significant proportion of these patients are discharged with residual congestion, which has been associated with an increased risk of mortality and readmission for heart failure. (8) However, the assessment of residual congestion in the pre-discharge phase remains a significant clinical challenge, as conventional methods, such as physical examination and chest X-ray, exhibit considerable interobserver variability and low sensitivity. (9)
In this regard, objective assessment of the patient’s volume status is essential for optimizing both treatment and follow-up after hospital discharge. Several studies have demonstrated the value of echocardiography and pulmonary ultrasound in revealing anatomical and physiological abnormalities in patients with AHF, and when correctly applied, they can improve patient assessment, management, and outcomes during follow-up. (10-12) However, there is limited information regarding their application in the elderly population of our setting.
Therefore, the objective of this study was to evaluate the prognostic utility of these methods in a cohort of elderly patients with “pure” heart failure-without secondary causses-in order to identify those at higher risk of readmission and/or death following discharge for AHF.
METHODS
Study design and population
A prospective, consecutive cohort study was conducted including patients over 65 years of age hospitalized for AHF between December 2022 and December 2024, in a healthcare organization comprising a university hospital and outpatient centers. Patients with de novo AHF or decompensated chronic heart failure admitted to the Cardiac Intensive Care Unit were included in the study.
Patients with acute coronary syndrome, severe valvular heart disease requiring surgery, a history of heart transplantation, Takotsubo syndrome, acute myocarditis, and congenital heart disease were excluded. These exclusions were established due to differences in the pathophysiology and therapeutic management of the aforementioned conditions. Similarly, pulmonary diseases that could limit obtaining an adequate ultrasound window, such as pulmonary fibrosis, advanced chronic obstructive pulmonary disease (GOLD C/D), acute respiratory distress syndrome, or acute parenchymal infectious processes were excluded.
Follow-up was conducted for six months following hospital discharge. Data sources included the institutional electronic medical records and administrative databases.
Methods and image analysis
Transthoracic echocardiography and lung ultrasound (LUS) studies were performed at hospital admission (within the first 12 hours) and prior to discharge (within the preceding 24 hours).
For echocardiography, measurements were performed following standardized protocols recommended by international guidelines. (13,14) In the case of LUS, the simplified 4-zone protocol described by Platz et al. was used for B-line quantification. (12) All images were acquired, analyzed, and interpreted by trained ultrasound staff.
Endpoint
The endpoint was a composite of mortality or readmission for AHF within 180 days of the index hospitalization. Outcome assessment was performed by an investigator blinded to the results of the transthoracic echocardiogram and LUS.
Mortality: all-cause mortality within 180 days following the index hospitalization.
Hospitalization for AHF: first readmission due to AHF, characterized by a hospital stay of more than 6 hours in the Cardiac Intensive Care Unit or the Emergency Department, caused by a worsening of signs and/or symptoms of heart failure requiring intravenous diuretic therapy.
Statistical analysis
Consecutive sampling was used, including all eligible patients. Sample size calculation was performed to estimate the accuracy of the area under the ROC curve (AUC). Considering an expected AUC of 0.8 and a margin of error (difference between the true and estimated AUC) of 0.08 with a 95% confidence level, the estimated number of patients required was 200.
Continuous variables were described using mean and standard deviation (SD) or median and interquartile range (IQR), depending on the distribution. Categorical variables were expressed as absolute and relative frequencies.
Bivariate associations were evaluated using Student’s ttest or the Wilcoxon test for continuous variables, and the chi-square test or Fisher’s exact test for categorical variables, as appropriate. Correlation was assessed using Spearman’s correlation coefficient. A ROC curve analysis was performed to evaluate the ability of the B-line count to separate patients who presented with the composite endpoint. The optimal cutoff point to simultaneously maximize sensitivity and specificity was selected using the Youden index. Multivariate Cox proportional hazards models were used to estimate prognostic factors for the outcome. The hazard ratio (HR) and its 95% confidence interval were reported. The assumption of proportional hazards and the goodness of fit were evaluated.
Values of p <0.05 were considered statistically significant, using two-tailed tests. Statistical analysis was performed using STATA software version 13.1 (StataCorp LP, College Station, TX).
RESULTS
Baseline characteristics
The study included a total of 200 patients. Baseline characteristics are presented in Table 1. Median age was 81 years (IQR 76-86), and 53% were men. The most prevalent comorbidities were hypertension (85%), dyslipidemia (58%), history of heart failure (51%), chronic kidney disease (43%), and atrial fibrillation (44%). Additionally, 28% of patients had diabetes mellitus at the time of inclusion.
Table 1
Baseline characteristics
| Characteristic | n=200 |
|---|---|
| Age - years (median, IQR) | 81 [76-86] |
| Male sex - n (%) | 106 (53) |
| Hypertension - n (%) | 170 (85) |
| Dyslipidemia - n (%) | 116 (58) |
| Diabetes mellitus - n (%) | 56 (28) |
| Coronary heart disease - n (%) | 65 (32.5) |
| Prior functional class (NYHA) - n (%) | |
| I | 102 (51) |
| II | 89 (44.5) |
| III | 6 (3) |
| IV | 3 (1.5) |
| Chronic kidney disease - n (%) | 86 (43) |
| History of heart failure - n (%) | 103 (51.5) |
| Atrial fibrillation - n (%) | 89 (44.5) |
| Medication - n (%) | |
| ACEI/ARB | 88 (44) |
| Beta-blockers | 138 (69) |
| MRA | 30 (15) |
| Sacubitril/valsartan | 6 (3) |
| SGLT2i | 41 (20.5) |
| Furosemide | 83 (41.5) |
| NT-proBNP - pg/mL (median, IQR) | 6515 [3077-14202] |
| LVEF - % (mean ± SD) | 44 ±14 |
ARB 2: angiotensin II receptor blockers; ACEI: angiotensin-converting enzyme inhibitors; IQR: interquartile range; LVEF: left ventricular ejection fraction; MRA: mineralocorticoid receptor antagonists; NT-proBNP: N-terminal pro-B-type natriuretic peptide; SGLT2i: sodium-glucose cotransporter 2 inhibitors.
Characteristics of hospital stay
Pulmonary and/or systemic congestion was the most frequent clinical presentation, observed in 77% of cases, followed by acute pulmonary edema (21%) and low cardiac output syndrome (2%). On physical examination at admission, the predominant findings were pulmonary crackles (89%) and lower limb edema (72%). Median serum N-terminal pro-B-type natriuretic peptide (NT-proBNP) level at admission was 6515 pg/mL (IQR 3077-14 202).
Among the echocardiographic variables measured at admission, several parameters are noteworthy. Mean left ventricular ejection fraction (LVEF) was 45% ± 14% (Simpson method). Regarding diastolic dysfunction parameters, mean septal and lateral E/e’ ratios were 19 ± 7 and 16 ± 6, respectively; monophasic filling was observed in 48% of patients, and mean left atrial volume index was 58 ± 18 mL/m². A dilated inferior vena cava (IVC) (>20 mm) with inspiratory collapse <50% was observed in 67% of patients. In addition, mean TAPSE recorded was 19 ±3.7 mm and mean pulmonary artery systolic pressure (PASP) was 47 ±15 mmHg. In the case of significant valvular heart disease (moderate grade or greater), mitral regurgitation was the most common finding (39%), followed by tricuspid regurgitation (32%). At discharge, some echocardiographic variables showed no significant changes (LVEF, TAPSE, and left atrial index volume).
In contrast, septal and lateral E/e’ ratios decreased to 14 ±6 and 11 ±5, respectively, PASP decreased to 40 ±14 mmHg, and the percentage of patients with dilated IVC without significant inspiratory collapse decreased to 8%. However, 29% of cases presented with a dilated IVC and significant inspiratory collapse at discharge.
On LUS, the median number of B-lines at admission was 13 (IQR 11-18), and it decreased to 4 (IQR 2-8) at discharge (p < 0.001), with a difference between admission and discharge of 9 (IQR 7-11).
Finally, median length of hospital stay was 5 days (IQR 3-7).
Post-discharge follow-up and variables associated with the incidence of the endpoint at 180 days
Median follow-up was 5.3 (IQR 2.9-5.9) months. The endpoint occurred in 75 patients (37.5%), comprising 25 deaths and 50 rehospitalizations for AHF.
A significant correlation (p < 0.001) was observed between the number of B-lines at discharge and established prognostic variables such as NTpro-BNP at admission (r = 0.22) and at discharge (r = 0.46). Significant, albeit weaker, correlations were also found with LVEF (r = 0.13) and left atrial volume (r = 0.19). No significant associations were identified between the number of B-lines and sex, age, or chronic kidney disease.
In the univariate analysis, the echocardiographic variables obtained at hospital discharge that were associated with the endpoint were the septal (HR 1.04; 95% CI 1.03-1.11) and lateral (HR 1.12; 95% CI 1.07-1.17) E/e’ ratio, IVC dilation (HR 6.1; 95% CI 3.6-10.35), PASP (HR 1.03; 95% CI 1.02-1.05), and TAPSE (HR 0.87; 95% CI 0.81-0.95).
In contrast, LVEF (HR 0.99; 95% CI 0.97-1.01) and left atrial index volume (HR 1.00; 95% CI 0.99-1.01) showed no association with the outcome.
The number of B-lines at discharge was significantly associated with the endpoint in the univariate analysis (HR 1.28; 95% CI 1.19-1.37). Association with the endpoint was also found for the absence of significant weight loss (HR 1.18; 95% CI 1.10-1.27), the presence of crackles (HR 2.46; 95% CI 1.55-3.94), and the persistence of lower limb edema (HR 3.65; 95% CI 2.31-5.76) at discharge.
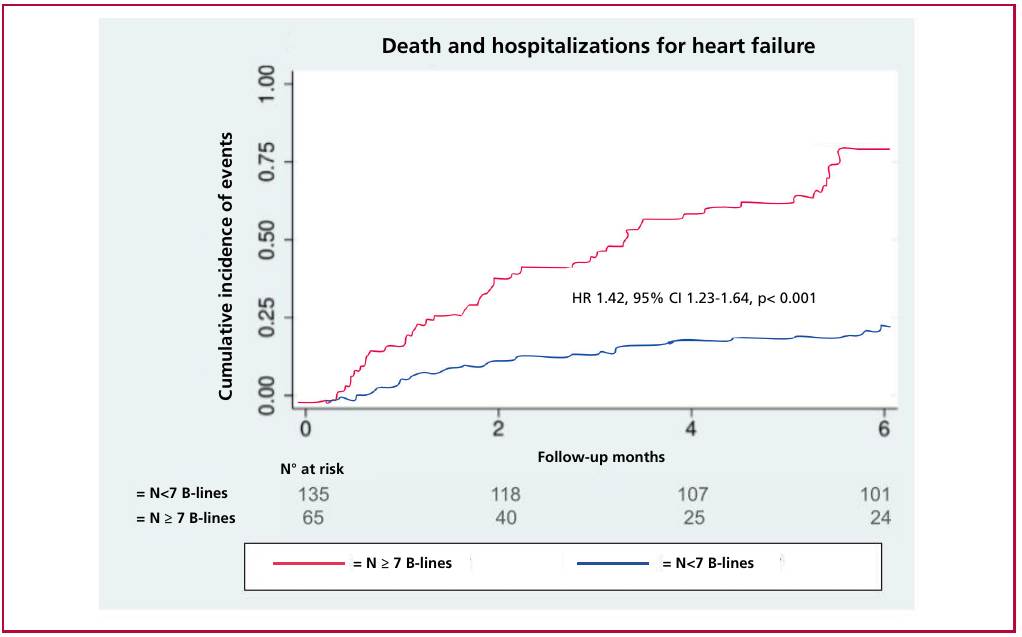
In the multivariate analysis, the number of B-lines was the only variable included that showed a significant association with the endpoint (HR 1.42; 95% CI 1.23-1.64). Table 2 shows the model results, including the ultrasound variables measured at discharge, and the cumulative incidence of readmissions or death at 180 days.
Table 2
Echocardiographic variables measured at discharge associated with the cumulative incidence of readmissions or death at 180 days
| Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Male sex | 0.82 (0.52-1.29) | 0.945 | 1.59 (0.83-3.06) | 0.166 |
| Age | 1 (0.98-1.02) | 0.805 | 0.99 (0.97-1.01) | 0.765 |
| B-lines | 1.28 (1.19-1.37) | <0.001 | 1.42 (1.23-1.64) | <0.001 |
| Septal E/e’ ratio | 1.07 (1.03-1.11) | <0.001 | 1 (0.92-1.02) | 0.264 |
| Lateral E/e’ ratio | 1.12 (1.07-1.17) | <0.001 | - | - |
| Dilated inferior vena cava | 6.1 (3.6-10.3) | <0.001 | 2 (0.91-4.53) | 0.080 |
| TAPSE | 0.88 (0.81-0.95) | 0.002 | - | - |
| LVEF | 0.99 (0.97-1.01) | 0.316 | 0.99 (0.96-1.01) | 0.474 |
| PASP | 1.03 (1.02-1.05) | <0.001 | 1.01 (0.99-1.03) | 0.254 |
LVEF: left ventricular ejection fraction; PASP: pulmonary artery systolic pressure; TAPSE: tricuspid annular plane systolic excursion.
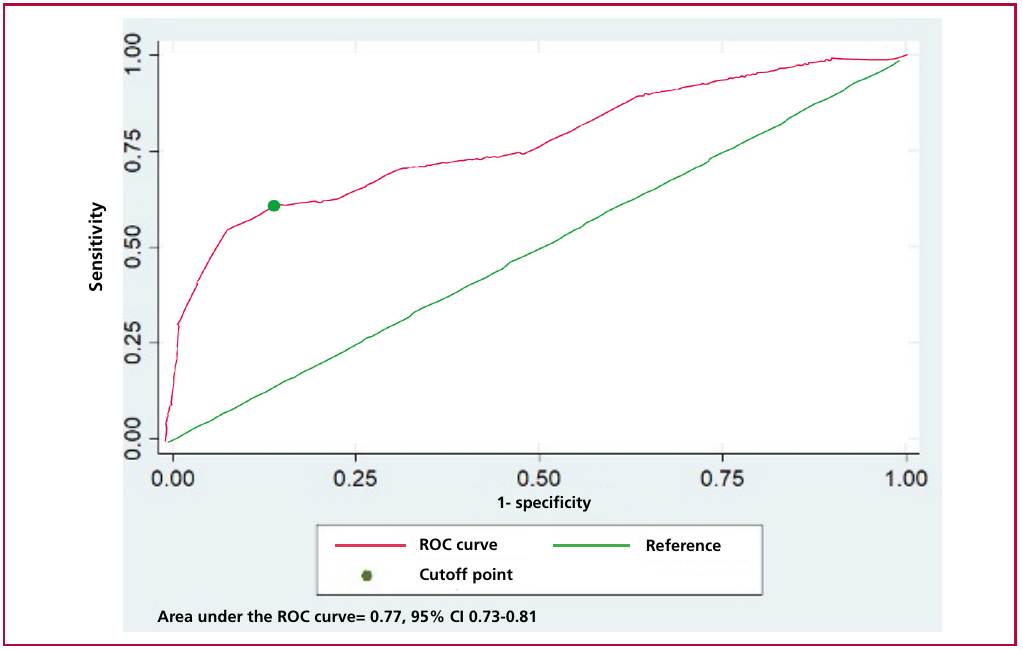
Finally, ROC analysis revealed an AUC of 0.77 (95% CI 0.73-0.81) of B-lines at discharge for endpoint discrimination (Figure 1). The optimal cutoff point was ≥7 B-lines, with a sensitivity of 61% and specificity of 86%, a positive predictive value of 73%, and a negative predictive value of 79%. The cumulative incidence of events among the groups with the highest and lowest number of B-lines according to this cutoff point is presented in Figure 2 (p<0.001, Log-rank test).
Fig. 1
ROC analysis revealed an area under the curve (AUC) of 0.77 (95% CI 0.73-0.81) for B-lines at discharge to discriminate the endpoint. The optimal cutoff point was ≥7 B-lines, with 61% sensitivity and 86% specificity.
DISCUSSION
In light of current published data, this is the first study to evaluate the prognostic value of echocardiography combined with a simplified LUS method in an elderly population with “pure” AHF. We suggest naming it this way because we excluded secondary causes of HF-such as acute myocardial infarction or severe valvular heart disease requiring surgery-that could alter therapeutic management and prognosis. This characteristic constitutes the main difference compared with other cohorts in which this restriction was not applied in patient selection. (12, 17-19) It should be noted that our research group had previously conducted a validation study of LUS in a study with a smaller number of patients and the same selection criteria. (20)
One of the main findings of our study was that one-third of patients hospitalized for AHF experienced the composite endpoint of rehospitalization or death within 180 days of the index admission. This high incidence is consistent with reports by other authors, (21) confirming the poor prognosis of AHF and underscores the need to identify patients with residual congestion prior to hospital discharge.
Compared with other AHF registries, such as the ADHERE, (22) and OPTIMIZE-HF (23) studies and various Argentine registries, (24) our cohort had a 10-year older median age. Although age distribution was similar to that of an Italian cohort, our population showed a higher prevalence of female patients, kidney failure, and prior history of heart failure. (25)
As previously mentioned, although there is evidence that patients with residual pulmonary congestion prior to hospital discharge are at higher risk of adverse events related to heart failure, there is no universally accepted definition of residual congestion assessed by echocardiography and pulmonary ultrasound that has prognostic value in older adults.
In our study, echocardiographic variables-septal and lateral E/e’ ratios, TAPSE, IVC assessment, and PASP-and the presence of B-lines on pulmonary ultrasound at hospital discharge were observed as predictors of the endpoint.
The E/e’ ratio is a widely used parameter for assessing diastolic function. Its prognostic value has been extensively evaluated in other conditions such as acute myocardial infarction (26), hypertension (27), or atrial fibrillation. (28) In the field of heart failure, we can highlight studies that obtained conclusive results regarding the prognostic use of this variable, although they were conducted in a population with heart failure with reduced ejection fraction (HFrEF). (29) On the other hand, in patients with preserved ejection fraction (HFpEF), the study by Blanco et al., conducted at our institution in 2020, is worth noting. Following an analysis of diastolic dysfunction parameters in AHF, these authors concluded that an E/e’ ratio greater than 14 measured at hospital discharge was significantly associated with the composite endpoint of all-cause mortality and readmissions for AHF (HR 4.63, 95% CI 2.71-18.2; p < 0.001). (30) Finally, Santas et al. conducted an analysis in a group of patients with AHF that included both HFrEF and HFpEF and demonstrated an independent association between elevated E/e’ values and all-cause mortality. (19) Regarding the similarities between our study and the latter, we note that our population also included both HFrEF and HFpEF. The main difference lies in the patients’ age: the mean age in the cited study was 72 years, whereas our median age exceeds it by 10 years, showing a substantially older population.
On the other hand, to compare our results from the IVC analysis, it is relevant to highlight the PROFUND-IC Registry. (31) This study evaluated the prognostic impact of LUS and IVC in a cohort of elderly patients with AHF, a population comparable to ours. The authors demonstrated that IVC collapsibility <50% or a diameter >2.25 cm was associated with increased short-term mortality, with greater predictive power than B-line quantification. A relevant methodological difference was the timing of the assessment: in the aforementioned registry, it was performed within the first 72 hours of hospitalization, whereas in our cohort, the measurements analyzed were taken at the time of hospital discharge.
The association between TAPSE, PASP, and the endpoint reflects the leading role of the right ventricle in this patient group. (32) It is known that right ventricular (RV) dysfunction is present in 4-50% of patients with heart failure and is a variable indicating poorer prognosis. (33-35) Several studies have reached similar conclusions when analyzing each of these parameters separately. (17, 36)
Regarding LUS, previous studies have identified several cutoff values for B-lines with prognostic significance, depending on the protocol used and the clinical context (12,31) Imanishi et al. investigated the correlation between the number of B-lines on LUS and pulmonary capillary pressure (PCP) and found that a count of ≥6 B-lines was strongly correlated with elevated PCP values and associated with a higher risk of cardiac death and rehospitalization for AHF. (37) Similarly, we found that the identification of ≥7 B-lines at discharge was associated with an increased risk of death or rehospitalization during follow-up. Furthermore, the adoption of a simplified LUS protocol, such as the one used in this study, is beneficial in the hospital setting due to its shorter execution time and lower risk of data omission. This is particularly relevant in count-based quantification methods, in which the total number of B-lines in all evaluated areas is added. Additionally, although AHF can present with different clinical phenotypes, most patients exhibit some degree of pulmonary congestion, (38) which supports the usefulness of pulmonary ultrasound in assessing the state of decongestion. In this regard, all patients in our cohort presented with B-lines at admission. Finally, it is worth noting that we decided to prioritize the assessment at discharge in our analysis, rather than relying on measurements taken at admission and the admission-to-discharge variation. This choice was based on its greater feasibility in routine clinical practice, as it requires a single measurement.
Our findings highlight the prognostic value of echocardiography combined with pre-discharge LUS in patients hospitalized for AHF. Both methods represent a potential therapeutic target for decongestion, showing that different variables analyzed by both methods exhibit dynamic changes during hospitalization, with rapid positive changes in patients who respond to diuretic therapy and other interventions. Serial LUS, for its part, has proven to be an effective modality for guiding the titration of diuretic therapy, facilitating early resolution of congestion, and potentially contributing to a shorter length of hospital stay. (39) Further research is needed to evaluate the impact of both methods as therapeutic guides during hospitalization for AHF in order to achieve optimal decongestion, which could result in a lower incidence of adverse events during follow-up.
This study has several limitations that should be acknowledged. First, it was conducted at a single high-complexity center, which may limit the generalization of the findings to other healthcare settings or to populations with different clinical characteristics and access to care. Second, the multivariate model was developed to assess prognostic factors; therefore, we cannot establish causality. Third, although ultrasound is widely regarded as a highly useful noninvasive tool, it is operator-dependent, even when standardized protocols are used. Fourth, the exclusion of NT-pro-BNP in the multivariate model should be emphasized. This decision was based on two considerations: the limited number of events available to include additional variables in the model and, even more importantly, the priority of developing a clinical model that is feasible to apply in less complex centers at lower costs.
Future studies should validate these findings in multicenter cohorts and explore interventions based on them to improve clinical outcomes during followup.
CONCLUSION
A comprehensive ultrasound approach that includes parameters such as the E/e’ ratio (septal and lateral), PASP, TAPSE, IVC assessment and B-lines provides useful information prior to discharge of older adults hospitalized for AHF.
The main findings of our study were: a) one-third of patients hospitalized for AHF presented the composite endpoint of rehospitalization or death within 180 days of the index admission. b) several echocardiographic variables (septal and lateral E/e’ ratios, TAPSE, IVC assessment, and PASP) and the presence of B-lines on the pulmonary ultrasound at hospital discharge were associated with the primary endpoint. c) The optimal cutoff point for B-lines at discharge to predict the endpoint was ≥7.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web).