
INTRODUCTION
Obstructive sleep apnea syndrome (OSAS) is a complex disease with multiple symptoms and associated comorbidities, characterized by the intermittent presence of apneas and hypopneas, i.e. total or partial obstruction of the airway, during sleep. This leads to a state of hypoxemia, autonomic fluctuation, and sleep fragmentation. (1)
Daytime and nocturnal symptoms or cardiometabolic comorbidities are caused by obstructive sleep apnea (OSA). Both terms (OSA and OSAS) are often used interchangeably in the literature. (2)
The estimated prevalence of this disease is 3% in women and 10% in men between 30 and 49 years of age, and 9% in women and 17% in men between 50 and 70 years of age, (3) but among patients with hypertension (HTN), heart failure (HF), atrial fibrillation (AF), coronary heart disease, pulmonary hypertension and stroke, the prevalence increases significantly. (4)
Most patients are unaware of the disease and, what is worse, do not consider sleep disturbances relevant, so they do not consult and are not diagnosed.
Currently, OSA is recognized as a problem that generates a high cost to health systems worldwide. The aim of this review is to understand the pathophysiology, its importance as a risk factor and its relationship with cardiovascular disease (CVD).
Pathophysiology
The pathophysiology of OSA is the result of the interaction between alterations in upper airway anatomy and upper airway function during sleep.
Morphologic abnormalities are the most common factors contributing to upper airway obstruction (e.g., retrognathia, enlarged tonsils, and increased soft tissue in the neck). In patients with decompensated HF, jugular distention during supine decubitus may exacerbate OSA by increasing pressure in the hypopharynx. (5)
Regarding the pathophysiological effects on the cardiovascular system, apnea-hypopnea episodes cause periodic hypercapnia and hypoxemia, with activation of the sympathetic nervous system and elevation of serum catecholamines. Both factors increase heart rate and systolic blood pressure, and thus myocardial oxygen consumption. Similarly, frequent awakenings and lack of sleep due to periodic asphyxia also activate the sympathetic nervous system. (6) Over time, these hemodynamic changes eventually lead to left ventricular hypertrophy and HF. In addition, hypoxemia promotes oxidative stress, systemic inflammation and endothelial dysfunction, contributing to the development of atherosclerotic disease. To counteract pharyngeal narrowing, negative intrathoracic pressure is generated, which increases mechanical stress on the cardiac chambers. This generates remodeling, with left ventricular hypertrophy and left atrial enlargement. These maladaptive changes may manifest as diastolic failure and AF.
Epidemiology and factors contributing to OSA
Obstructive sleep apnea is a common disorder in adults, and its prevalence has increased with the increasing presence of obesity. It is highly predominant in populations with diabetes, hypertension, heart disease, and stroke. Environmental factors also contribute to the risk of OSA. The epidemiology of OSA depends on the criteria used to diagnose the disease, including how respiratory events are defined, apnea- hypopnea index (AHI) cutoff points, and how diagnostic tests are performed. The criterion of arterial oxygen saturation (SaO2) drop ≥ 4 % for hypopneas may have greater association with patients who are older, male, obese, and have underlying cardiac disease (e.g., HF, coronary artery disease, AF, or diabetes). The American Academy of Sleep Medicine (AASM) defines hypopneas more broadly (desaturation ≥3 % or awak- ening) and allows the inclusion of more variable sleep disturbance phenotypes seen in younger, non-obese, and female patients. (2)
A meta-analysis of 17 studies estimated that 936 million adults aged 30-69 years worldwide suffer from mild to severe OSA, with prevalence exceeding 50% in some places. (7) The prevalence of OSA is associated with gender, obesity, and age. It is higher in men (2:1), but rates increase in women after menopause, and become nearly equal in older adults. Prevalence increases with age, particularly in those over 60 years of age.
Obesity is the main modifiable risk factor for OSA. There is an association between OSA and increased waist circumference and neck circumference (with increased prevalence of OSA in those with values >43 and 41 cm in men and women, respectively). (2)
Craniofacial anomalies that narrow the upper airway or increase airway collapsibility may explain the occurrence of severe OSA despite the absence of obesity. Other less well-established risk factors include smoking, family history of OSA, and nocturnal nasal congestion.
The use of substances such as alcohol or benzodiazepines can exacerbate pre-existing OSA. (4)
Clinic
The signs and symptoms of OSAS are summarized in Table 1.
Table 1
Clinical manifestations and association with physical examination in obstructive sleep apnea syndrome (OSAS).
| Signs and Symptoms Physical examination | |
|---|---|
| Excessive daytime sleepiness | Obesity |
| Morning headaches | Increased neck circumference |
| Memory impairment | Craniofacial abnormalities |
| Irritability | |
| Problems with concentration | |
| Nocturia | |
| Erectile diffusion and decreased sexual desire | |
Diagnosis and detection of OSA
Obstructive sleep apnea is usually suspected on the basis of symptoms and confirmed by diagnostic tests, which may be performed by a home sleep apnea study, multichannel polysomnography, or overnight laboratory testing.
Laboratory polysomnography is the gold standard for the diagnosis of OSA, but it can be expensive and difficult to access.
Validated questionnaires can be a quick tool to stratify patient risk.
The diagnosis requires:
1) reported nocturnal breathing disorders (snoring, snorting, gasping, or pauses in breathing during sleep) or symptoms of daytime sleepiness or fatigue that are not explained by other medical conditions.
2) an AHI ≥5 episodes/hour.
OSA can be diagnosed in the absence of symptoms if AHI is ≥15 episodes/hour. Empirical categorization is based on AHI from: 5 to <15 (mild), 15 to 30 (moderate), and >30 (severe). (8)
Recent research has identified hypoxia burden as a predictor of increased CVD risk. (9)
The detection of this pathology is done by questioning the patient, which should include questions about the frequency and severity of snoring, gasping and snorting during sleep, frequent awakenings or sleep interruptions, and excessive daytime sleepiness. The most commonly used screening questionnaires are the STOP-BANG questionnaire (Table 2), the Berlin questionnaire (Table 3), and the STOP questionnaire. (10) These questionnaires sensitivity is between 77% and 89%, but have lower specificity (32%-34%). The use of the Epworth sleepiness scale is not recommended, as it has higher specificity (67%) but low sensitivity (42%). (10)
Table 2
STOP-BANG Questionnaire
| Item evaluated | Finding |
|---|---|
| Snoring | Snoring loudly (more than talking or loud enough to be heard through a closed door). |
| Tiredeness | Often fatigue or daytime sleepiness |
| Observed | Observed to stop breathing during sleep |
| Blood Pressure | High blood pressure or current treatment for hypertension |
| BMI | >35 kg/m2 |
| Age | >50 years |
| Neck circumference | >40 cm |
| Gender | Male |
≥ 3 or 4 findings= high risk of OSA
< 3 findings= low risk for OSA
BMI: body mass index; OSA: obstructive sleep apnea
Table 3
Berlin Questionnaire
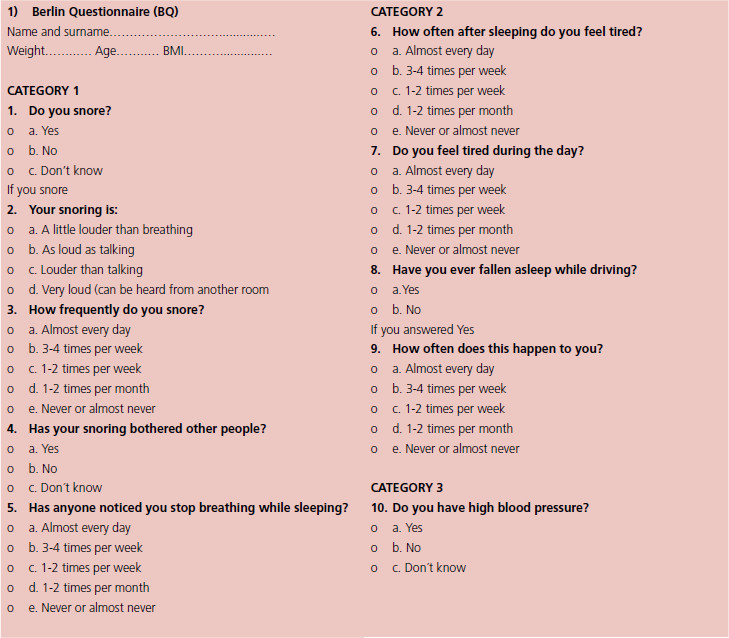
Berlin Score
Category 1 (positive ≥ 2 points). -Questions 1-4 = 1 point each. Question 5 = 2 points
Category 2 (positive ≥ 2 points)- -Questions 6-8 = 1 point each.
Category 3 (positive if BMI is > 30Kg/m2 or there is HTN
High risk = 2 positive categories (positive Berlin)
Low risk = ≤ 1 positive category (negative Berlin)
BMI: body mass index; HTN: hypertension
On the other hand, given the strong association between OSA and numerous cardiovascular conditions, screening is recommended in patients with:
-
Resistant or poorly controlled HTN, pulmonary arterial hypertension (PAH) and recurrent AF.
-
NYHA FC II to IV HF, with suspected sleep breathing disorders or excessive daytime sleepiness.
-
Tachycardia-bradycardia syndrome, ventricular tachycardia or sudden death survivors and suspected sleep disturbances.
-
Angina of nocturnal occurrence, myocardial infarction, arrhythmias or appropriate discharges from implantable cardioverter defibrillators.
-
History of stroke
Cardiovascular consequences
Obstructive sleep apnea is an independent risk factor for CVD. It is also recognized to be associated with metabolic disorders, closely related to cardiovascular diseases. While sleep fragmentation and respiratory stress are contributing factors to OSA-associated pathologies, several clinical studies associate AHI with cardiovascular events. Furthermore, intermittent hypoxia, which mimics the repetition of oxygen saturation-desaturation cycles, has been shown to be the main mechanism responsible for OSA-associated cardiovascular and metabolic complications. (11)
Cardiovascular complications include HTN, AF and other arrhythmias, HF, coronary artery disease, stroke, PAH, metabolic syndrome, diabetes, and cardiovascular mortality. It is a condition with negative feedback potential, exacerbating disorders that in turn may worsen OSA.
The relationship between OSA and hypertension has been extensively investigated and there is convincing evidence that there is a dose-effect relationship between the severity of OSA and the degree of blood pressure (BP) elevation. (12)
The pathophysiological mechanisms by which OSA contributes to BP elevation are multifactorial. On the one hand, OSA-induced hypoxemia causes systemic inflammation and oxidative stress, resulting in increased endothelin-1 generation and decreased nitric oxide production in endothelial cells, increased arterial peripheral resistance, and elevated BP. On the other hand, periodic hypoxemia, frequent awakenings and lack of sleep cause activation of the sympathetic nervous system, which leads to increased cardiac output and peripheral vasoconstriction, and thus promotes BP elevation. Patients with OSA have a higher prevalence of isolated diastolic HTN and the underlying mechanism could be due to tachycardia and shortening of diastole. Compared with subjects without OSA, subjects with OSA also have greater activation of the renin angiotensin system. Taken together, these effects lead to an elevation of BP due to vasoconstriction and sodium and water retention. In addition, primary hyperaldosteronism is very prevalent in subjects with OSA, highlighting the importance of screening them for primary hyperaldosteronism. These patients are more likely to develop drug-resistant HTN. Finally, sleep deprivation due to OSA has been shown to be associated with endothelial dysfunction and arterial stiffness. (13)
Adherence to continuous positive airway pressure (CPAP) is associated with greater reductions in nocturnal BP.OSA and atrial fibrillation share many risk factors and comorbidities (male sex, HTN, congestive HF, coronary artery disease). The presence of OSA has been shown to predict pre-discharge AF after coronary revascularization surgery. In addition, untreated OSA doubles the risk of AF recurrence in patients after electrical cardioversion, and treatment of OSA with CPAP attenuates that risk. (14,15)
Multiple possible mechanisms can trigger AF in patients with OSA, but underlying to hypoxia and hypercapnia. Altered intrathoracic pressure generates increased sympathetic tone and autonomic dysregulation. This may lead to structural and functional atrial remodeling and cause electrophysiological alterations. (16)
Treatment of AF is more difficult in these patients. In the ORBIT-AF trial, patients with OSA had significantly worse symptoms, even though they were under rhythm control therapy. People with OSA had more episodes of recurrent AF, even after catheter ablation. Treatment of OSA is indispensable for the proper management of AF and maintenance of sinus rhythm. The cohort of patients treated with CPAP in the ORBIT-AF trial were less likely to progress to persistent AF compared with those who did not receive such treatment. Moreover, other trials have demonstrated less AF after catheter ablation in patients with OSA treated with CPAP compared with a risk of up to 57% AF recurrence in those not treated with CPAP. (17,18) Although it seems reasonable to optimize sleep quality to avoid complications such as AF, to date there is no evidence to support the use of CPAP to prevent AF. The SAVE study failed to demonstrate significant differences in patients treated with CPAP vs. control. (19,20)
In addition to AF, OSA is associated with other cardiac rhythm disturbances and sudden cardiac death. These include sinus pauses, ventricular tachycardia and first-degree atrioventricular block. Nocturnal hypoxemia is independently a strong predictor of sudden death. In general, patients experience a reduction in cardiac arrhythmias when treated with CPAP. (21)
Obstructive sleep apnea and heart failure share numerous risk factors and pathophysiological mechanisms, which together may contribute to HF progression or refractoriness to treatment. Obstructive sleep apnea has a high prevalence and is associated with adverse outcomes in patients with HF, related to hospitalization and mortality. There is also an increased risk of central sleep apnea in these patients.
Obstructive sleep apnea is more frequent in HF patients with reduced left ventricular ejection fraction (LVEF), with an estimated prevalence ranging between 12% and 53%.
Although confirmatory studies are lacking, it is postulated that OSA may adversely affect HF patients through several mechanisms. Heart failure is a state of sympathetic overactivity in addition to the autonomic imbalance associated with OSA in response to hypoxemia, which may generate concomitant physiological stress. Moreover, the rise in intrathoracic pressure due to inspiratory effort exerts an increase in transmural pressure in the heart and great vessels, leading to increased afterload, reduced stroke volume, and higher myocardial oxygen consumption. (22)
Considering these pathophysiological mechanisms, CPAP therapy would be expected to have benefits in patients with HF. In addition to improving airway obstruction in OSA and reducing inspiratory effort, CPAP decreases venous return (preload) and may attenuate sympathetic activity. However, these physiological benefits have not yet translated into improved clinical outcomes in patients with OSA and HF. (23, 24)
In patients with HF and central sleep apnea, continuous positive airway pressure is associated with improved sleep quality and nocturnal oxygenation but has not been shown to affect survival. (25)
Regarding coronary artery disease, the prevalence of OSA in patients presenting with acute coronary syndromes (ACS) is up to 69%. In addition, OSA has been associated with an increased risk of adverse events after ACS. (6)
Intermittent hypoxia and concomitant increased sympathetic activity, inflammation, endothelial dysfunction, and elevated blood pressure are associated with higher risk of cardiovascular morbidity and mortality. Obstructive sleep apnea has been associated with coronary artery calcification, plaque instability, and vulnerability. During obstructive apneas, increased adrenergic tone and hypoxemia may increase the risk of myocardial ischemia. (2)
Patients with suspected OSA who present with ACS are more likely to be male and have conventional risk factors. On admission, these patients have higher levels of BP, C-reactive protein, and B-type natriuretic peptide (BNP), all of which are long-term predictors of CV morbidity and mortality. (6) Obstructive sleep apnea has also been associated with an increased risk of adverse events after percutaneous coronary intervention (PCI) for ACS. One study followed-up 89 consecutive patients after PCI for ACS for a mean of 227 days. The incidence of major adverse events (cardiac death, reinfarction, and revascularization of the treated vessel) was significantly higher in patients with OSA (23.5% vs. 5.3%). (26)
Whether CPAP therapy reduces the risk of myocardial infarction is still debated, and the timing of starting treatment in the acute setting is a point of discussion.
Obstructive sleep apnea is highly prevalent (55%) among hemorrhagic stroke patients and significantly increases the risk of ischemic stroke. (27)
It also increases the risk of stroke through a variety of factors that lead to vascular damage in the brain. Repeated hypoxia can cause damage to the endothelium and release of proinflammatory factors, such as plasma cytokines, tumor necrosis factor-alpha, and interleukin-6. This may ultimately cause vascular dysfunction by increasing endothelin, neurovascular oxidative stress, and susceptibility to injury. (2)
Untreated OSA in stroke patients can cause cognitive impairment, decreased concentration, and excessive daytime sleepiness, which may prolong hospital stay and hinder rehabilitation. (28)
Trials with CPAP in post-stroke patients, despite their difficult follow-up, have shown promise for stroke recovery and secondary prevention. (29)
The prevalence of OSA is as high as 70% to 80% among patients with pulmonary arterial hypertension diagnosed by right heart catheterization. (30) Obstructive sleep apnea should always be ruled out because of 3 conditions: it is associated with higher mortality; it requires adjustment of the appropriate treatment; and due to the possibility of coexistence with other PAH etiologies that might require different treatment strategies.
Although the mechanism behind PAH associated with OSA is not fully understood, it is postulated to be due to a combination of factors including pulmonary arteriolar remodeling, susceptibility to hypoxia, and underlying left heart disease. (31)
A study of WHO group I PAH patients showed that there was no significant difference in mortality between patients with and without OSA; however, mortality was significantly higher in patients with nocturnal hypoxemia, suggesting that the duration and severity of oxygen desaturation, characteristic of OSA, is an important risk factor for the development of PAH. (32)
Although data on the effect of CPAP on hemody namic variables have been inconsistent, some reviews conclude that CPAP therapy is associated with a re duction in mean pulmonary artery pressure (mPAP) in patients with OSA and PAH. (33,34)
Although CPAP appears to improve hemodynamic variables including mPAP and systolic PAP in patients with OSA and PAH, the mechanisms are still unclear. As we know, in the context of metabolic syndrome and type diabetes, the severity of insulin resistance is directly related to nocturnal hypoxia in
non-obese patients with OSA.
Alterations in lipid metabolism are also observed in patients with OSA.
The desaturation index, another indicator of the severity of nocturnal hypoxia, has been identified as an independent contributor to hypercholesterolemia and hypertriglyceridemia. (35)
In patients with metabolic syndrome, the prevalence of moderate to severe OSA is very high, around 60%. In this population, OSA is independently associated with increased glucose and triglyceride levels, as well as markers of inflammation, arterial stiffness and atherosclerosis. (36, 37) Although CPAP has been shown to reduce blood pressure and markers of sympathetic activation, it has not been shown to affect lipid levels, glycemic control, or rates of metabolic syndrome or diabetes. (1)
Prognosis
Moderate and severe OSAS are associated with an increased risk of vascular complications and all-cause mortality. This relationship may differ between genders. (38) Observational studies have shown a significant reduction in mortality with positive airway pressure, with greater risk reduction observed among patients with HF. However, large randomized controlled trials have not yet demonstrated an effect of positive airway pressure, including CPAP, on survival.
(24) In an analysis of the Sleep Heart Healthy Study, CPAP prescription was associated with 42% lower mortality among patients with severe OSAS, but this risk reduction was not observed until 6 to 7 years of follow-up. (39)
Treatment
There are numerous treatment options for OSA. (5) Lifestyle intervention and weight loss of 10% reduces AHI by 26%.
Continuous PAP treatment during sleep is indicated with AHI ≥15, or ≥5 with symptoms (daytime sleepiness, cognitive impairment, mood disorders or insomnia), or comorbidities (hypertension, ischemic heart disease or history of stroke).
The objective is to avoid airway collapse with constant positive inspiratory and expiratory pressure. It requires a nocturnal laboratory titration study and an adherence of 40-80 % (4 hs or more per night) during 70% of the period of use is defined.
Continuous PAP treatment showed improvement in somnolence, blood pressure and quality of life. Sometimes there is intolerance to the treatment due to problems of adaptation to the mask, claustrophobia, nasal congestion, or dry mouth or nose.
In patients intolerant to CPAP therapy or requiring additional ventilatory support, bilevel positive airway pressure (BiPAP) therapy is a treatment alternative since it allows the use of different inspiratory and expiratory pressures and is useful in patients who cannot tolerate high expiratory pressures. Adherence is similar to that of CPAP (40-80 %). (40)
Adaptive servoventilation (ASV) may be an option for OSA, especially in cases where apnea persists or is complicated by central apnea in the absence of HF (LVEF <45 %). (41)
Positional therapy is indicated in cases of isolated events, or predominantly in supine position (AHI is twice as high in the supine position than that in the lateral decubitus position). In selected patients it has a similar efficacy to CPAP. Long-term adherence is low (10%) due to discomfort.
Oral appliances are an alternative to CPAP for mild to moderate obstructive apneas. Adherence is generally higher than for CPAP, and as with CPAP, there is improvement in sleepiness, ambulatory blood pressure and markers of inflammation. They should be prescribed by a physician and adjusted by a qualified dentist.
Upper airway surgery is an acceptable alternative on occasions when there are multiple levels of obstruction and collapse.
Finally, bariatric surgery in patients with body mass index ≥35 kg/m2, may improve OSA in addition to its multiple metabolic benefits. (42)
CONCLUSIONS
Obstructive sleep apnea is a growing health problem affecting nearly one billion people worldwide, and is an independent cardiovascular risk factor.
The cardiovascular and metabolic comorbidities associated with this entity are a major concern, due to the worsening prognosis and the complexity of integrated treatment.
Intermittent hypoxia, a characteristic factor of OSA, is the key intermediary mechanism underlying metabolic and cardiovascular complications.
Understanding the molecular pathways involved in the metabolic and cardiovascular consequences of OSA is a priority for new pharmacological tools, in combination with, or as an alternative to continuous positive pressure.
Continuous positive airway pressure, first-line therapy for the treatment of OSA, is very effective in improving symptoms and quality of life, but has limited effect on comorbidities. Lifestyle changes and weight loss should be part of the treatment whenever indicated.
The current literature clearly points to OSA as an emerging risk factor for modulating the cardiometabolic consequences of cardiovascular disease. However, OSA is commonly underdiagnosed.
There are several challenges. We need to do more screening for OSA in patients with both cardiovascular disease and traditional risk factors. There is need to provide a cost-effective way to perform adequate screening and diagnosis of OSA in millions of patients with other manifestations. Portable monitoring and new technologies for OSA diagnosis are promising options in high-risk groups, as full polysomnography may not be readily available.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web/Additional material).