
We report the case of a 69-year-old female patient with a history of neuroendocrine tumor of the colon with liver metastases and episodic diarrhea. She completed chemotherapy with everolimus and sunitinib. During follow-up, she presented with 24-hour urinary 5-hydroxyindoleacetic acid (5-HIAA) levels of 136 mg (normal value: 2-8 mg) and plasma chromogranin levels of 241 ng/mL (normal value: 19-98 ng/mL). The patient was admitted due to FC IV dyspnea, edematous syndrome and fatigue lasting more than one month. On physical examination the liver was enlarged, and ascites was present.
On transthoracic color-Doppler echocardiography (TTE), the left ventricular (LV) and right ventricular (RV) diameters and wall thickness were preserved. There was global LV hypokinesia and the ejection fraction (EF) was 36%. The left atrium was mildly dilated and the right atrium exhibited marked dilatation. The mitral valve had moderate regurgitation. The tricuspid valve leaflets were thickened, presented increased refringence suggestive of fibrosis with reduced opening and there was low implantation of the valvular plane with moderate regurgitation. The estimated systolic pulmonary artery pressure was 55 mm Hg and there was severe pulmonary valve regurgitation and an atrial septal aneurysm 2 L of the Olivares Reyes classification (Figure 1 A and B).
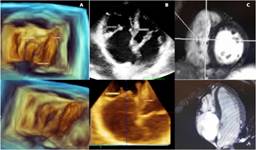
Figure 1
A. Three-dimensional transthoracic echocardiogram (TTE) images of the stenotic tricuspid valve from the right ventricular view. The septal leaflet is thickened, adhered to the interventricular septum and fused with the posterior leaflet. The anterior leaflet is significantly thickened. B. Top: Two-dimensional echocardiography images in the apical 4-chamber (4C) view showing thickened tricuspid valve with reduced valve opening. Bottom: Three-dimensional echocardiography images in the apical 4C view showing thickened tricuspid valve with reduced valve opening. C. Cardiac magnetic resonance imaging (MRI). Fast imaging employing steady-state acquisition (FIESTA). Tricuspid valve stenosis is observed in the short-axis sequence and four-chamber sequence.
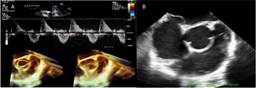
The transesophageal echocardiography (TEE) revealed increased transvalvular gradient across the tricuspid valve and thickening of the tricuspid subvalvular apparatus. The pulmonary valve was thickened, flail and retracted, lacking valve leaflet coaptation, and had increased velocities with severe regurgitation (Figure 2).
Figure 2
A. Transesophageal echocardiography (TEE) with color-Doppler imaging of the pulmonary valve with increased transvalvular gradient and severe regurgitation. Three-dimensional TEE images showing a thickened and retracted pulmonary valve in systole and diastole. B. M-mode image of the pulmonary valve by transthoracic Doppler echocardiography at the level of the great vessels. The pulmonary valve is thickened and retracted.
On cardiac magnetic resonance imaging (MRI) LV end-diastolic volume (EDV) was 32mL/m2, end-systolic volume (ESV) was 22 mL/m2 and the EF was 32%, with global hypokinesia and LV mass of 42 g/m2. Right ventricular EDV was 34ml/m2, ESV was 15 mL/m2 and the EF was 65%. The left atrial volume was 65 mL and the right atrial volume was 75 mL. The LV walls presented intramyocardial edema in IR T2 and Triple IR sequences (Figure 1 C). The IR sequences showed non-ischemic gadolinium enhancement in the LV, with linear septal intramyocardial and epicardial distribution, and in the RV insertion zone, both atria, mitral valve and tricuspid valve.
Multimodality imaging exhibited findings suggestive of carcinoid heart disease, with involvement of both the tricuspid and pulmonary valves in a patient with ventricular dysfunction undergoing chemotherapy.
Carcinoid tumors are rare, with an incidence between 1.2 to 2.1 per 100 000 in the general population. Carcinoid heart disease occurs in about one third of patients with carcinoid tumors (particularly ileal carcinoid) with liver metastases and may be the initial manifestation. Cardiac involvement is characterized by the presence of an endocardial plaque comprised of fibrous tissue, resulting in valvular thickening and regurgitation. This carcinoid plaque is composed of muscle cells, myofibroblasts, extracellular matrix and an overlying endothelial cell layer. These deposits occur most commonly in the endocardium of the valve cusps. (1) Left-sided heart involvement does not occur in these patients, except in those with bronchial carcinoid or right-to-left shunts.
The most common finding on TTE is tricuspid valve involvement in approximately 90% of cases, with severe regurgitation and mild or moderate stenosis. The pulmonary valve is also commonly affected (50 to 69%) and shows similar changes in valve regurgitation or stenosis. (2) TEE allows for high-resolution images of the tricuspid valve with the fixed triangular orifice and thickened subvalvular apparatus. The use of multiplanar reconstruction (MPR) for planimetry of the tricuspid valve area in systole and diastole provides a quantitative measure of tricuspid regurgitation and tricuspid stenosis, presenting opportunities for the evaluation and monitoring of disease severity and progression. (3)
When TTE is anatomically inconclusive, cardiac MRI and/or CT scan may be performed.
Cardiac MRI is useful for risk stratification prior to treatment, surveillance, diagnosis and follow-up of cardiotoxic therapy, long-term effects, screening after treatment completion, and evaluation and follow-up of cardiac masses and infiltration. It also identifies the presence of myocardial edema, inflammation, and global and focal fibrosis. (4,5)
This patient is currently under joint evaluation with the Department of Oncology to assess the therapeutic course of action in the new scenario where double valve replacement surgery has been proposed as an effective strategy. (6)
Ethical considerations
Not applicable.
Declaración de conflicto de interés
None declared. (See authors' conflict of interests forms on the web).