
INTRODUCTION
Hypertension (HTN) is the most relevant modifiable cardiovascular risk factor (CVRF) due to its frequency and association with cardiovascular morbidity and mortality. One of the key terms associated with HTN is “HTN-mediated organ damage” (HMOD), which describes how the presence of HTN subclinical complications are indicators of a higher risk of serious clinical events in the future, such as heart failure or chronic kidney disease. (1,2) Hypertension is defined as systolic blood pressure (SBP) ≥140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg at the medical consultation. For an accurate diagnosis, it is recommended to take at least two measurements at different visits, or to confirm the elevated values with complementary ambulatory studies, such as ambulatory blood pressure monitoring at home (ABPM) or 24-hour ambulatory monitoring. These measurements provide a more reliable description of the patient's hypertensive status outside the clinical setting, where blood pressure (BP) can vary due to external factors. (3)
In recent years, there has been a notable increase in the prevalence of HTN in young adults (YA), both men and women. This increase has been promoted by factors such as unhealthy lifestyles (poor diet, sedentarism, and alcohol and tobacco consumption), obesity, and unfavorable socioeconomic conditions. These factors contribute to a higher risk of developing HTN at younger ages, which in turn increases the long-term risk of cardiovascular disease. In fact, the impact of HTN in terms of mortality or years of life lost due to disability has increased especially in low- and middle-income countries, where resources for diagnosis and treatment may be limited. (4)
It is important to note that both systolic and diastolic HTN, and even isolated diastolic HTN, are associated with an increased risk of cardiovascular events (CVE) in YA, an age group that has traditionally been considered at lower risk. However, this risk is often underestimated, as awareness of HTN, its treatment, and control is considerably lower in YA compared with older age groups. This phenomenon contributes to underdiagnosis and insufficient treatment in this population, which increases the likelihood of mid- and long-term cardiovascular complications. (5,6)
METHODS
A cross-sectional observational design with prospective follow-up was carried out, evaluating patients who attended a cardiovascular health prevention program (HPP) at Fundación Favaloro University Hospital. The HPP is designed to assess general health, counsel and educate on healthy lifestyle habits, and detect patients at high cardiovascular risk (CVR). Patients between 18 and 49 years of age who attended for cardiovascular (CV) assessment between January 2017 and December 2023 were included. Anthropometric, clinical, and laboratory data were collected from medical records. Waist circumference (WC) was measured with a non-extensible tape measure at a midpoint between the lower edge of the ribs and the iliac crests with the patient standing in normal expiration and body mass index (BMI) was calculated: weight/height2: kg/m2). BMI allowed patients to be divided into normal weight (<25 kg/m2), overweight ( ≥25- 30 kg/m2) and obese ( ≥30 kg/m2).
Diabetes mellitus (DM) was defined as the presence of two fasting blood glucose (FBG) measurements ≥126 mg/dL or treatment with insulin or oral hypoglycemic agents ; (7) dyslipidemia in the following circumstances: low-density lipoprotein cholesterol (LDL-c) ≥190 mg/dL, high-density lipoprotein cholesterol (HDL-c) <40 mg/dL for men or <50mg/dL for women, total serum triglycerides (TG) ≥150 mg/dL, or being medicated with lipid-lowering drugs; current smoking defined as patients who had smoked at least one cigarette in the last 6 months and more than 100 cigarettes throughout their lives; and family history of atherosclerotic cardiovascular disease, as having first-degree relatives and manifestations before the age of 55 years in men and 65 years in women. (8) High blood pressure was considered for SBP ≥140 mmHg or ≥90 mmHg for DBP in the medical consultation . Metabolic syndrome (MS) was diagnosed according to the criteria of the National Cholesterol Education Program - Adult Treatment Panel III (NCEP-ATP III). (9) The components of MS were defined as follows: 1) high BP (SBP ≥130 mmHg and/or DBP ≥85 mmHg or taking antihypertensive medication); 2) elevated WC (>102 cm for men and >88 cm for women); 3) hyperglycemia (FBG ≥100 mg/dL or hypoglycemic treatment); 4) hypertriglyceridemia (TG ≥150 mg/dL); and 5) low HDL-c (<40 mg/dL for men and <50 mg/dL for women). Metabolic syndrome was considered to be present with at least 3 of the components described.
A color Doppler echocardiogram was performed using an Affinity 50 ultrasound system (Philips HealthCare, USA) to evaluate the left atrial structure (LA) and calculate left ventricular mass index (LVMI). A graded exercise test was used to assess the hypertensive response to exercise (SBP ≥210 mmHg or DBP ≥90 mmHg).
The characteristics of the hypertensive group (HTNg) were compared with those of the normotensive group (control group, CTRLg). Patients with previous HTN, under treatment with antihypertensive drugs, or with secondary HTN were excluded.
Statistical analysis
Quantitative variables were expressed as mean±standard deviation (SD) or median and interquartile range (IQR), according to the normal distribution evaluated by the Kolmogorov-Smirnov test. Qualitative variables were expressed as number and percentage. Comparisons between groups were performed using Student's t-test or Mann Whitney test for continuous variables and the Chi2 test or Fisher's exact test for categorical variables. A multiple logistic regression analysis was performed to test the independent association between HTN and other CVRF. Variables with a known biological relationship or those with statistically significant differences in the univariate analysis (age, gender, BMI, FBG, HDL-c, TG, LA diameter, LVMI, and exaggerated hypertensive response in the ergometric test) were employed for the model. A two-tailed p-value <0.05 was considered statistically significant. Statistical analysis was performed using SPSS software version 16 (SPSS Inc, Chicago, Illinois, USA) and R version 4.3.1. This study was approved by the institutional bioethics committee.
RESULTS
Among a total of 6071 participants who met the inclusion criteria (age 35.3±9.6 years, and 45.3% female), 576 patients (9.5%) had elevated BP values during the medical consultation. The comparative data for this population, showing that patients in the HTNg had more unfavorable clinical characteristics compared with the CTRLg, are summarized in Table 1.
Table 1
Total population characteristics, with normal or high blood pressure at consultation. Quantitative variables are presented as mean ± standard deviation or median and interquartile range, according to their distribution
| Variable | Total | Normal BP at Consultation | HTN at consultation | p value |
|---|---|---|---|---|
| (n=6071) | (n=5495) | (n=576) | ||
| Age (years) | 35.3 ± 9.6 | 34.9±9.7 | 38.9±8.5 | <0.001 |
| Female sex (%) | 43.5 | 46.6 | 32.3 | <0.001 |
| Body mass index (kg/m2) | 26.8 ± 14 | 26.5±14.4 | 30.5±6.8 | <0.001 |
| Diabetes mellitus (%) | 58 (0.9) | 49 (0.9) | 9 (1.6) | 0.115 |
| Active smoking (%) | 1167 (19.2) | 1058 (19.2) | 109 (18.9) | 0.911 |
| Blood glucose (mg/dL) | 92,2 ± 16,6 | 91,8 ± 15,4 | 96,2 ± 25,1 | <0,001 |
| Creatinine (mg/dL) | 0.86 ± 0.16 | 0.86±0.16 | 0.89±0.17 | <0.001 |
| Total cholesterol (mg/dL) | 189.7 ± 37.6 | 188.8±37.4 | 198.7±32.6 | <0.001 |
| HDL-c (mg/dL) | 54.4 ± 13.5 | 54.8±13.6 | 50.7±11.9 | <0.001 |
| LDL-c (mg/dL) | 113.1 ± 32.8 | 112.4±32.6 | 120.5±33.7 | <0.001 |
| Triglycerides (mg/dL) | 92 (67-132) | 90 (66-128) | 115 (83-168) | <0.001 |
BMI: body mass index; BP: blood pressure; HDL-c: High density lipoprotein cholesterol; HTN: hypertension; LDL-C: Low density lipoprotein cholesterol
Qualitative variables are presented as percentages and quantitative variables as mean ± standard deviation or median and interquartile range,
according to their distribution.
In the HTNg, patients had older age, greater BMI, higher FBG levels, and elevated creatinine concentrations. In addition, lipid parameters, including total serum cholesterol, LDL-c, HDL-c, and TG, also showed significant alterations in this group of patients, reinforcing the relationship between HTN and other CVRFs.
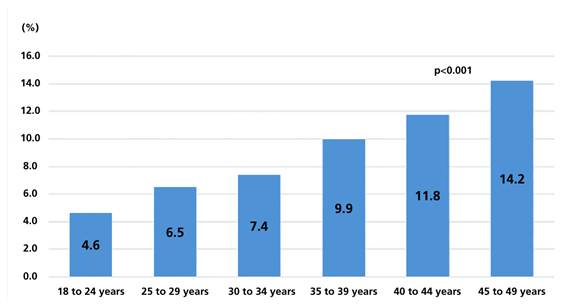
Regarding specific findings in the HTNg, 73.8% had elevated SBP, 91.1% had high DBP, and 64.9% had both elevated pressures. There was a strong relationship between increasing age and high BP, as can be seen in Figure 1.
Fig. 1
Percentage of patients with elevated blood pressure values at the consultation according to the age group
On the other hand, the results of the ergometric test, an assessment of physical performance during exercise, indicated that the HTNg patients showed significantly lower performance, measured in METS (metabolic equivalents) compared with the CTRLg. On average, HTNg patients reached 12.2±2.8 METS, while normotensive patients reached 13±2.8 METS (p<0.001). In addition, the probability of an exaggerated hypertensive response during exercise was statistically much higher in the HTNg compared with normotensive individuals:8.3% vs. 1% (p<0.001).
Another relevant finding was the increase in LVMI in the HTNg (66±16g/m² vs. 62.5±14.5g/m², p<0.001) suggesting a greater hemodynamic load in hypertensive patients. Similarly, patients in the HTNg had a statistically significant larger anteroposterior LA diameter (35.9±5 mm vs. 33.9 ± 4.9mm in the CTRLg, p<0.001).
Multiple logistic regression analysis revealed that several factors were independently associated with the presence of HTN in the consultation. Age (OR 1.049, 95% CI 1.034-1.065), HDL-c (OR 0.985, 95% CI 0.973-0.996), triglycerides (OR 1.002, 95% CI 1.000-1.003), LA diameter (OR 1.048, 95% CI 1.019-1.078) and hypertensive response on the stress test (OR 8,897, 95% CI 5,151-15,367) were independently associated with the presence of HTN. (Table 2)
Table 2.
Variables associated with the finding of arterial hypertension. Multiple logistic regression.
| Variable | OR | 95% CI | p |
|---|---|---|---|
| Age | 1.049 | 1.034-1.065 | <0.001 |
| Male gender | 0.793 | 0.592-1.064 | 0.122 |
| BMI | 1.004 | 1.000-1.008 | 0.069 |
| FBG | 1.001 | 0.995-1.007 | 0.789 |
| HDL-c | 0.985 | 0.973-0.996 | 0.009 |
| TG | 1.002 | 1.000-1.003 | 0.010 |
| LA diameter | 1.048 | 1.019-1.078 | 0.001 |
| LVMI | 0.999 | 0.990-1.007 | 0.745 |
| Hypertensive response on the stress test | 8.897 | 5.151-15.367 | <0.001 |
BMI: body mass index; FBG: fasting blood glucose; HDL-c: high density lipoprotein cholesterol; LA: left atrium; LVMI: left ventricular mass index; OR: odds ratio; TG: triglycerides; 95% CI: 95% confidence interval
DISCUSSION
Hypertension is the most common modifiable CVRF with the greatest impact on CV health. In recent years, various factors, such as unhealthy lifestyles, greater obesity, and sedentarism, have contributed to the increase in the incidence of HTN in younger populations. (10,11) Our findings show an important number of young individuals with HTN, which is significantly associated with the presence of other CVRFs, such as dyslipidemia, obesity, and DM. What is worrying about these findings is that the diagnosis of HTN in young people, which is often underestimated or delayed, and the lack of adequate treatment, can have a severe impact on long-term CV health. Traditionally, youth has been considered to confer a certain degree of protection against CVE. However, our results suggest the opposite: age, in this context, does not always act as a protective factor, and subclinical damage can progress silently if early intervention is not provided.
The prevalence of HTN in people under 50 years of age has shown a steady increase in recent decades. New studies, such as the analysis of the National Health and Nutrition Examination Survey (NHANES) conducted between 2017 and 2020, reported a prevalence of 11.5% HTN in YA between 20 and 44 years of age. (12) Moreover, other publications have highlighted that the prevalence increases with age, and it has been observed that HTN affects approximately 14.5% of adults between 18 and 49 years of age. (13) These data reflect the growing burden of CVRF among YA, including obesity, sedentarism, and poor diet. In Argentina, the RENATA 2 study showed a prevalence of 18.5% HTN for men and 6.9% for women under 35 years of age, and between 37.9% and 19.5% among those aged 36 to 44 years old. (14) Espeche et al. also showed that this worrying situation could be magnified in vulnerable populations in Argentina. (15) In this context, our data coincide in revealing a high prevalence of elevated BP in the clinic.
In this population of YA, detection of HTN in the clinic was associated with an increase in LVMI which is a well-known significant marker of CVR in patients with HTN. (16,17) Schilacci et al. demonstrated that LVMI was continuously related to an increased risk of CVE. (18) It is interesting to remark that in this study, age, male sex, and a LVMI in the upper quintile were independent predictors of cardiovascular morbidity and mortality. Our interpretation is that this link is showing early signs of incipient target organ damage, which should be taken into account in the management of these patients. Another important finding is the presence of enlarged LA diameter. This echocardiographic finding is generally associated with increased left ventricular end-diastolic pressure, representing an atrial adaptation to pressure overload. The presence of LA enlargement has been associated with the incidence of CVE in YA. (19) Particularly in young patients with HTN, the presence of an enlarged LA increases the risk of stroke. (20) This relationship could be explained by increased blood stasis and the consequent formation of clots, although it is also suspected that atrial enlargement may be promoting the onset of atrial fibrillation. (21,22) Regardless of whether an exact cause can be established, the presence of increased LA diameter as an independent predictor in the multivariate analysis, is an alarming finding in this population of young patients.
The exaggerated response to the stress test was also a distinctive pattern associated with elevated BP during the consultation. This phenomenon has also been widely described previously. In a study by Yzaguirre et al., it was observed that the exaggerated response of SBP or DBP to moderate load (100W) is an independent predictor of future development of essential HTN. (23) In our population, the probability of presenting an exaggerated BP response was 8 times higher in participants with HTN at the medical consultation, which was also associated with reduced exercise test performance. We consider this to be another characteristic of these patients that should be noted for close follow-up and eventual early treatment.
We must consider some limitations of this study. First, it was conducted in a single center population, which may have influenced our results. In addition, the participants have health coverage and may represent a socioeconomic bias, which we recognize as very relevant when addressing the issue of HTN and CVRF. Even with these limitations, we think our population reflects the reality that many physicians face in their regular office care when they find high BP.
CONCLUSION
In conclusion, our findings are consistent with other reports of an increase in the prevalence of HTN in YA. The association with other CVRF and the presence of HMOD are an additional concern and a warning for the care of this population. Improving detection, prevention, and early treatment strategies are priorities for preventing early CVE. Future studies with long-term follow-up and measurement of CVE may define the benefit of early detection of CVRF, together with an appropriate preventive and therapeutic approach to avoid future complications and reduce the burden of CV disease in the general population
Declaración de conflicto de interés
Los autores declaran no tener conflicto de intereses. (Véase formularios de conflictos de interés de los autores en la Web).