
INTRODUCTION
Atrial fibrillation (AF) is the most frequent sustained cardiac arrhythmia in adults, and its prevalence has been increasing over the past decades due to aging population and increased survival from other cardiovascular diseases. (1) It is associated with an increased risk of thromboembolic events, (2) cognitive impairment, (3) heart failure, hospitalizations, and death. (4)
In turn, it is the most frequent arrhythmic complication in patients with acute coronary syndrome (ACS), and its incidence ranges from 2.3% to 21%. (5) In Argentina, the incidence of de novo AF in this setting is 3.2%, as observed in the ARGEN-IAM-ST registry. (6) Over the last decades and with the advances in invasive and medical treatment, its incidence has decreased. (6) Several studies have evaluated the clinical characteristics of patients with de novo AF after ACS. The main predictors were advanced age, signs of heart failure, and tachycardia on hospital admission. These predictors have been maintained both in studies performed in the fibrinolytic era and in the present day, when percutaneous treatment is available. (7, 8)
In the general population and in patients with ACS, the presence of AF is associated with a worse prognosis. De novo AF in the setting of ACS is associated with increased morbidity and mortality. (9, 10) In turn, several observational studies have shown that patients with coexisting ACS and de novo AF are less likely to receive appropriate antithrombotic treatment. (11, 12) However, there is a lack of studies analyzing the predictors and prognosis of these patients in the setting of invasive and medical treatment, as recommended by the latest guidelines. This study aimed to evaluate the incidence of de novo AF during hospitalization for ST-elevation myocardial infarction (STEMI) and to determine the predictors associated with its development.
METHODS
Study design and population
This is an observational and retrospective study based on the analysis of the continuous registry of ST-segment elevation acute myocardial infarction (ARGEN-IAM-ST), which includes patients with STEMI from numerous centers in Argentina. Its protocol was previously published and has been active since 2015. (13,14) The protocol has been registered in ClinicalsTrials.gov under NCT 2458885. The cut-off date for the analysis of this work was May 2024.
Definitions and outcomes of interest
Our outcome of interest was de novo AF during hospitalization, defined as AF in patients who had an admission electrocardiogram (ECG) showing sinus rhythm and an episode of AF as a complication during their progress. This was modeled as a binary variable. We excluded from this definition those patients with a history of AF and atrial flutter.
Statistical analysis
Continuous variables are expressed as mean and standard deviation (SD) or median and interquartile range (IQR), according to their type of distribution. The variables of age and heart rate were analyzed by strata. Qualitative variables are expressed as absolute and relative frequencies. Qualitative variables were compared using the chi-square test or Fisher's exact test, while continuous variables with parametric and nonparametric distribution were compared using Student's t test and the Mann Whitney U test, respectively.
To reduce dimensionality and identify those variables associated with our outcome of interest, the Boruta Machine Learning algorithm was used. (15) To ensure that variable selection was stable and reproducible, the algorithm performed up to 50 iterations which allowed a robust assessment of the importance of each predictor in de novo AF ranking. In addition, its performance was monitored during the process to verify consistency in feature selection. Multivariate analysis using logistic regression was performed with the most important variables to identify the factors independently associated with de novo AF. The models were trained and evaluated on two different databases randomly generated from the general database. The performance of the models and their discrimination ability was evaluated through the generation of receiver operating characteristic (ROC) curves. Since the aim of the model was to maximize sensitivity to identify the greatest number of cases of de novo AF, the optimal cut-off point was selected from the ROC curve with the highest possible sensitivity criterion, while maintaining clinically acceptable specificity. The Hosmer Lemeshow test was used to evaluate the goodness of fit of the model. The association between the predictors and the incidence of events was expressed as odds ratio (OR) with their 95% confidence intervals (CI). In addition, a multivariate model was performed to explore de novo AF as an independent predictor of mortality. All tests were two-tailed and statistical significance was set at a p-value <0.05.
The analysis was performed with R Studio, version 1.4.1106 (The R Foundation for Statistical Computing, Vienna, Austria).
Ethical considerations
The ethics committee of the Argentine Society of Cardiology approved the protocol of the Argen IAM-ST registry.
RESULTS
Baseline characteristics of the population
We included a total of 7292 patients with STEMI and evidence of sinus rhythm on admission ECG, of which 79% were male, and had a median (IQR) age of 61 (53-69) years. Table 1 shows the baseline characteristics.
Table 1
Baseline clinical characteristics of participants with and without de novo AF
| Global | Without de novo AF | With de novo AF | p | |
|---|---|---|---|---|
| n | 7292 | 6974 | 318 | |
| Male gender, n (%) | 5754 (79) | 5512 (79) | 248 (78) | 0.705 |
| Age, years, median (IQR) | 61 (53-69] | 60 (53-68) | 67(60-77) | <0.001 |
| BMI, kg/m2, median (IQR) | 27.65 | 27.68 | 27.41 | 0.041 |
| (25.47-30.61) | (25.51-30.76) | (25.28-29.97) | ||
| DM, n (%) | 1980 (27.2) | 1900 (27.2) | 80 (25.2) | 0.451 |
| Smoking, n (%) | 591 (8.1) | 563 ( 8.1) | 28 ( 8.8) | 0.717 |
| DLP, n (%) | 2662 (36.5) | 2553 (36.6) | 109 (34.3) | 0.433 |
| HT, n (%) | 3870 (53.1) | 3661 (52.5) | 209 (65.7) | <0.001 |
| Previous coronary artery disease, n (%) | 897 (12.3) | 846 (12.1) | 51 (16.0) | 0.047 |
| Beta-blockers , n (%) | 3635 (50.0) | 3519 (50.5) | 120 (37.7) | <0.001 |
| ACEIs, n (%) | 3301 (45.4) | 3178 (45.6) | 129 (40.6) | 0.090 |
| Glycemia, mg/dL, median (IQR) | 135 (113-179) | 134 (113-177) | 153 (124-212.50) | <0.001 |
| Creatinine, mg/dL, median (IQR) | 0.97 (0.80-1.18) | 0.97 (0.80-1.17) | 1.08 (0.90-1.40) | <0.001 |
| Reason for PCI, n (%) | 0.949 | |||
| Primary | 5003 (91.1) | 4887 (70.1) | 207 (65.1) | |
| Pharmacoinvasive | 273 (5.0) | 646 (9.3) | 37 (11.6) | |
| Rescue | 154 (2.8) | 976 (14.0) | 45 (14.2) | |
| Elective | 59 (1.1) | 465 (6.7) | 29 (9.1) | |
| SBP, mm Hg, mean (SD) | 131 (29) | 132 (29) | 121 (29) | <0.001 |
| HR, bpm, mean (SD) | 80 (19) | 80 (18) | 86 (26) | <0.001 |
| Killip and Kimball, n (%) | <0.001 | |||
| A | 5485 (77.0) | 5456 (78.2) | 153 (48.1) | |
| B | 1024 (14.4) | 955 (13.7) | 90 (28.3) | |
| C | 100 (1.4) | 95 (1.4) | 8 (2.5) | |
| D | 516 (7.2) | 468 (6.7) | 67 (21.1) | |
| Door-to-balloon time, min, median (IQR) | 84 (47-147] | 91(50. 175] | 92. (51.25- 209.75] | 0.439 |
| Time window, min, median (IQR) | 230 (135-440) | 252.50 (146- 510) | 289.50 (162.25- 612.25) | 0.019 |
| Multi-vessel PCI in initial procedure, n (%) | 351 (6.4) | 360 (5.2) | 26 (8.2) | 0.026 |
| LVSF, n (%) | <0.001 | |||
| Normal | 2397 (37.4) | 2660 (38.1) | 75 (23.6) | |
| Mild impairment | 1842 (28.7) | 1994 (28.6) | 58 (18.2) | |
| Moderate impairment | 1397 (21.8) | 1466 (21.0) | 93 (29.2) | |
| Severe impairment | 774 (12.1) | 854 (12.2) | 92 (28.9) |
ACEIs: angiotensin-converting enzyme inhibitors; AF: atrial fibrillation; BMI: body mass index; bpm: beats per minute; DLP: dyslipidemia; DM: diabetes mellitus; HR: heart rate; HT: hypertension; IQR: interquartile range; LVSF: left ventricular systolic function; PCI: percutaneous coronary intervention;SBP: systolic blood pressure; SD: standard deviation
We identified that 4.3% of the sample patients had de novo AF during hospitalization. These patients were older than those with no de novo AF (median age 67 vs. 60 years; p <0.001). We found no differences between the groups related to body mass index (BMI), diabetes mellitus and dyslipidemia. However, 53.1% had arterial hypertension (HT), and the prevalence was higher in the group of patients who developed AF during hospitalization (65.7% vs. 52.5%; p <0.001). In turn, the history of coronary artery disease -which was present in 12.3% of the total sample- was also more frequent in the group with de novo AF (16% vs. 12.1%; p = 0.047).
Regarding reperfusion strategies in all patients, primary angioplasty was performed in 91%, a pharmacoinvasive strategy in 5%, rescue angioplasty in 2.8%, and elective angioplasty in 1.1%, with no significant differences between the study groups. However, multi-vessel angioplasty was performed in the initial procedure in a higher proportion of patients who developed AF during hospitalization. There were no significant differences in the treatment of the culprit vessel for AMI.
Regarding treatment with beta-blockers and angiotensin-converting enzyme inhibitors on admission, we found a lower use in patients with de novo AF, that is, 37.7% vs 50.5% (p = 0.001) and 40.6% vs.45.6% (p =0.090), respectively.
On hospital admission, those patients who developed AF had a higher heart rate (86 bpm vs. 80 bpm; p <0.001). Regarding laboratory tests, they had higher glycemia values, with a median (IQR) of 153 mg/dl (124-212) vs. 134 mg/dL (113-177), p <0.001, and higher creatinine values: 1.08 mg/dL (0.90-1.40) vs. 0.97 mg/dL (0.8-1.17), p <0.001.
This group of patients also had longer total ischemia time (medians 289 min vs. 252 min; p = 0.019), a more severe Killip and Kimball score (p <0.001) and lower left ventricular ejection fraction (LVEF) (p <0.001).
In-hospital events
The presence of de novo AF was associated with a higher incidence of ischemic stroke (2.5% vs. 0.8%; p = 0.002) and more days of hospitalization (medians 6 vs. 4 days; p <0.001). In-hospital all-cause death was also higher in the de novo AF group (23.3% vs. 8.2%; p <0.001) (Table 2).
Table 2
In-hospital events of participants with and without de novo AF.
| Global | Without de novo AF | With de novo AF | p | |
|---|---|---|---|---|
| n | 7292 | 6974 | 318 | |
| Reinfarction, n (%) | 123 (1.7) | 113 (1.6) | 10 (3.1) | 0.066 |
| Stroke, n (%) | 61 (0.8) | 53 (0.8) | 8 (2.5) | 0.002 |
| Cardiogenic shock, n (%) | 682 (9.4) | 576 (8.3) | 106 (33.3) | <0.001 |
| HF, n (%) | 967 (13.3) | 818 (11.7) | 149 (46.9) | <0.001 |
| In-hospital death, n (%) | 591 (8.1) | 563 (8.1) | 28 (8.8) | 0.717 |
| LOS, days, median (IQR) | 4 (3-6) | 4 [3-6] | 6 [4-11] | <0.001 |
AF, atrial fibrillation; HF, heart failure; IQR, interquartile range; LOS: length of stay
Selection of important variables
Using the Boruta algorithm, an automated selection was performed to identify the variables with the greatest importance in the prediction of de novo AF. In the analysis, the Killip and Kimball, heart rate and LVEF variables were identified as the most important, followed by gender, age, dyslipidemia, and creatinine. Figure 1 shows the means of importance of each variable in the ranking. Subsequently, these variables were included in the multivariate logistic regression model to evaluate their association with the outcome.
Fig. 1
Variables with the greatest importance in the prediction of de novo AF
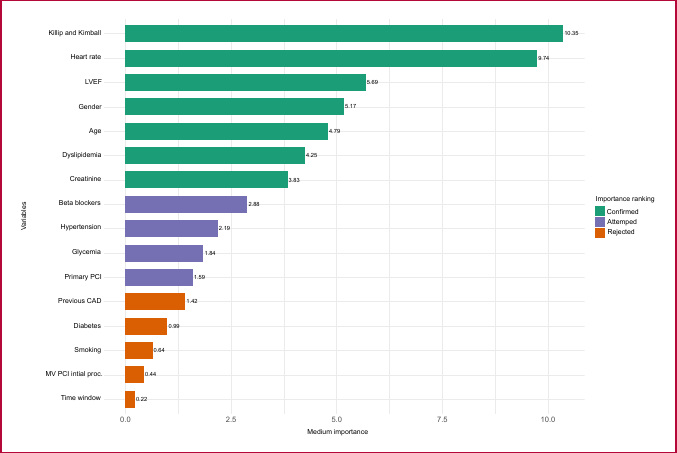
AF: atrial fibrillation; CAD: coronary artery disease; LVEF: left ventricular ejection fraction; MV: multiple vessels; PCI: percutaneous coronary intervention; proc: procedure; time window: time in minutes from symptom onset to start of infusion in the case of fibrinolytics or to balloon inflation in the case of PCI
Multivariate analysis: Independent predictors of de novo AF
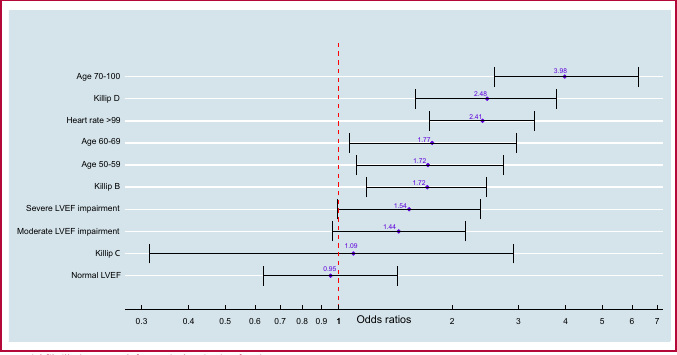
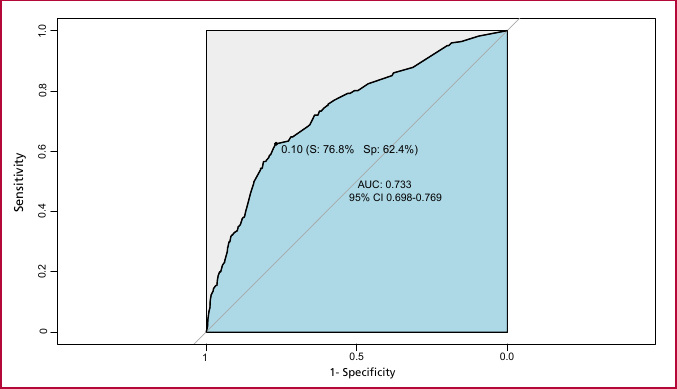
The greatest weight variables associated with de novo AF were included in a multivariate logistic regression model. The stratified age (50 to 59 years, 60 to 69 years, and 70 to 100 years) was independently associated with the incidence of de novo AF (OR 1.72, 95% CI 1.11-2.73; OR 1.77, 95% CI 1.07-2.96; OR 3.98, 95% CI 2.60-6.25, respectively). Clinical presentation according to Killip and Kimball score (B: OR 1.72, 95% CI 1.19-2.46; C: OR 1.09, 95% CI 0.315-2.90; D: OR 2.48, 95% CI 1.60-3.78), tachycardia (OR 2.41, 95% CI 1.74-3.31) and impaired LVEF (<35%) (OR 1.62, 95% CI 1.04-2.50) were also independent predictors (Figure 2). To evaluate the performance of the model, a ROC curve was constructed and the area under the curve (AUC) was 0.733 (95% CI 0.698-0.769). The optimal cut-off point was determined at 0.10 to maximize sensitivity. According to this threshold, the model correctly identified 77% of patients with de novo AF (sensitivity) and 62% of patients without de novo AF (specificity). This cut-off point represents the threshold where the balance between sensitivity and specificity is clinically most appropriate for the detection of de novo AF (Figure 3). The goodness of fit of the model, assessed by the Hosmer-Lemeshow test, was good (χ² = 5.33, p = 0.618).
Multivariate analysis: de novo AF as an independent predictor of mortality
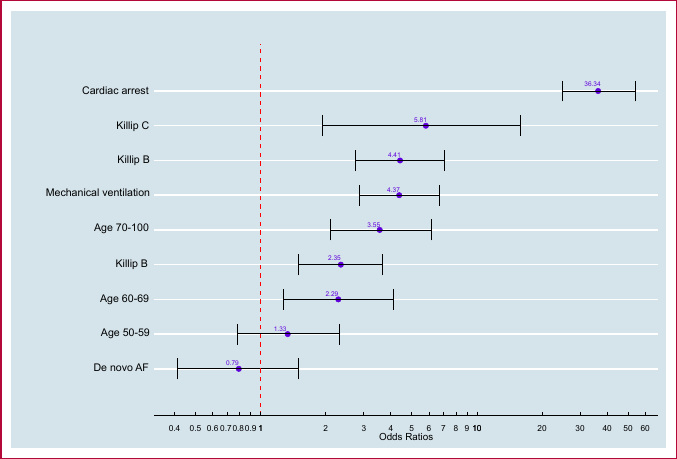
De novo AF was included with the main variables related to in-hospital mortality in a multivariate model. We observed that de novo AF did not behave as an independent predictor of in-hospital mortality (OR 0.79, 95% CI 0.41-1.50) (Figure 4).
DISCUSSION
We present data on the incidence of de novo AF during hospitalization for STEMI from the ARGEN-IAM-ST registry. On this occasion, cases with AF on admission ECG or with history of AF were excluded in order to evaluate the consequences of this event after AMI. The incidence of de novo AF was 4.3%, and the findings suggest an association with a greater number of in-hospital events and a longer hospital stay. In addition, certain factors such as age, heart failure assessed by the Killip and Kimball score, tachycardia, and impaired LVEF were shown to be independent predictors of de novo AF during hospitalization. These predictors were included in a ranking model to predict de novo AF, which showed an AUC of 0.733 (95% CI 0.698-0.769).
AF and ACS are two common heart diseases and, over the years, multiple studies have been performed to analyze the relationship between them. The risk of de novo AF increases by 60-77% in patients with AMI. (16) In the fibrinolytic era, the randomized GUSTO-I (1997) and GUSTO-III (2000) studies compared different fibrinolytic regimens in patients with STEMI, and highlighted a 7.9% and 6.5% incidence of de novo AF after ACS, respectively. (8, 17) In addition, OACIS, a prospective observational study published in 2003, analyzed patients with AMI (with and without ST-segment elevation) who underwent coronary angioplasty within 24 hours and found that the incidence of de novo AF was 7.7%. (18) Regarding national results, the incidence of in-hospital de novo AF in patients with AMI and unstable angina was 4.3% and 7.7%, respectively, according to data from the Buenos Aires I registry, which included patients with non-ST-elevation acute coronary syndrome (NSTE-ACS). (19) Similarly, a previous publication from the ARGEN-IAM-ST registry showed that the incidence of de novo AF was 3.2%, and the predictor factors were advanced age, history of HT and previous coronary artery disease. (6) There are definitely no randomized studies comparing the incidence of de novo AF in patients with STEMI treated with fibrinolytics versus primary angioplasty, and the differences in the populations and methods used in the published studies preclude a correct assessment of the incidence of this complication and whether the type of revascularization has an impact on it.
In our cohort, age acted as an independent predictor of de novo AF, with the higher impact observed specifically between the ages of 70 and 100 years, with an OR of 3.98. As AF outside the setting of ACS, age was closely related to the incidence of this arrhythmia. In one of the largest studies including only patients aged ≥65 years from the Cooperative Cardiovascular Project database published in 2000, (11) the rate of de novo AF after ACS was 22%, significantly higher than in studies including patients of all ages. In addition, the 2009 review by Schmitt et al., found that all studies published between 1992 and 2007 identified older age as an independent predictor of de novo AF after ACS. (20)
Although AF is the most frequent supraventricular arrhythmia in the general population, its incidence is significantly higher in patients with heart failure (HF). These two conditions are closely related to each other, and each perpetuates the presence of the other. (21) Our analysis showed that HF, as assessed by the Killip and Kimball score, was independently associated with de novo AF, as showed in the above mentioned GUSTO-I and III studies. Of note, a subanalysis of the international GRACE study, which included more than 21 000 patients with ACS and classified them according to the presence of de novo AF, previous AF, and no AF, identified a Killip score ≥2 as an independent predictor of de novo AF. (22) Similarly, tachycardia, probably secondary to HF, was also a predictor of de novo AF in our study and in the previously mentioned study. These results translate the impact of hemodynamic status within the pathophysiological mechanisms of AF in the setting of ACS and indicate that patients with altered hemodynamic status (HF, tachycardia, and/or hypotension) are at higher risk of AF.
In parallel, severely impaired LVEF (<35%) also functioned as an independent predictor of de novo AF in our analysis. Although the association between ventricular dysfunction and clinical presentation on admission (as reflected by the Killip and Kimball score and heart rate) is clear, other studies have not shown this variable to be an independent predictor of de novo AF.
LIMITATIONS
The registry ARGEN-IAM-ST is a voluntary participation registry with no audit strategy. Although a multivariate regression analysis was performed, we cannot completely exclude the possibility that unconsidered variables may have altered the results. Furthermore, although this is a multicenter study, it only represents the reality of the participating centers. Finally, it is not possible to determine when AF occurred during hospitalization, and thus the temporal relationship cannot be studied.
CONCLUSION
In this cohort of patients from the ARGEN-IAM-ST registry, de novo AF was a relatively frequent complication. Factors such as age, heart rate, hemodynamic profile on admission, and ventricular function were shown to be predictors of de novo AF after an AMI during hospitalization. However, de novo AF was not independently associated with in-hospital mortality.
Conflicts of Interest
None declared. (See the author’s conflict of interests forms on the Web).