
INTRODUCTION
Antarctica is the southernmost continent on Earth and one of the most hostile and inhospitable regions on the planet. Due to its geographic location and the tilt of the Earth's axis relative to the orbital plane, it receives less solar radiation, resulting in the low temperatures that characterize this continent, which can drop as low as -54 ºC during the winter. The climate is dry and there are strong winds. (1)
It has the cleanest air on Earth; it is an atmospheric region unaffected by human activity, and therefore, pollution carried by wind does not reach it.
Argentina occupies the territory known as the Argentine Antarctic Sector, which covers an area of approximately 1 461 597 km2. Within the Argentine territory, there are 13 bases. One of them, Belgrano II Base, the southernmost, is located 1300 km from the South Pole. It is considered one of the most isolated bases, with very extremely limited access, and reaching it from other bases can take several days. (Photograph).

It is occupied and maintained each year by personnel from the Joint Antarctic Command, who remain at the base for a full year (January to January). During this period, there is no personnel turnover or short-term visits. They perform tasks related to the base maintenance, domestic duties and scientific activities following an eight-hour work schedule (9 AM to 6 PM) from Monday to Friday, with fixed times for breakfast, lunch and dinner. The diet is devoid of vegetables and relies heavily on canned food.
One of the most notable characteristics of the Belgrano II Base is its extreme photoperiod, with four months of continuous darkness (polar night) and four months continuous daylight (polar day). These conditions make it an ideal natural setting for studying the influence of natural light on circadian rhythms. Light is considered one of the main synchronization sources of the central biological clock, and limited or absent light exposure can lead to innumerable disruptions in human physiological functioning. (2)
Belgrano II is considered one of the most challenging bases for overwintering, due to its weather conditions, extreme photoperiods, limited social interaction and isolation. It is one of the most required and internationally recognized bases for studying these variables, and represents one of the most faithful experimental scenarios as a spatial analog, since it combines multiple specific environmental characteristics rarely found together in other places.
Our objective was to investigate the cardiovascular function under conditions of circadian disruption, confinement and prolonged isolation, particularly in a low-pollution area.
METHODS
This was an observational, analytical and longitudinal study conducted at the Argentine Antarctic Belgrano II Base. A total of 23 trained and healthy military personnel were included in the study and sent to the base. All participants agreed to participate in the project.
Participants underwent body weight monitoring, abdominal waist circumference measurement and body composition analysis using bioelectrical impedance (OMRON® HBF-514C). The body, environmental and outdoor temperature were recorded.
Exercise stress test was performed using Cardiovex® equipment on a Technogym® cycle ergometer, which automatically calculates metabolic equivalents (METs) of oxygen consumption. Measurements included baseline and maximal effort (Mx. effort) blood pressure (BP), recovery BP at 1 and 3 minutes, achieved METs, and peripheral oxygen saturation (SpO2) at baseline and at maximal effort. The Astrand protocol was used, with ascending workload stages of 300, 600, 900, 1200, and 1500 kgm. The same protocol was applied to all subjects.
Additionally, a 24-hour Holter ECG (Eccosur HT107®) was performed to determine the heart beats per day, maximum and minimum heart rate (Max. and Min. HR), heart rate variability (Standard Deviation of Normal-to-Normal (NN) intervals, SDNN) and the presence of arrhythmias.
Measurements were made in March (baseline), June, July, August (months of darkness) as well as in October, November and january (months of daylight).
Baseline results were compared with those from both darkness and daylight periods, and darkness and daylight periods were also compared with each other.
Statistical analysis
A Generalized Estimating Equations (GEE) approach was used to assess the variations in the ergometric variables in the different evaluation timepoints. GEE allows modeling the correlation between repeated measurements from the same subject, thus allowing comparisons across time. Model validity was assessed using two types of correlation matrices: exchangeable or -1 autocorrelation. The exchangeable matrix assumes a similar correlation among all measurement pairs, while the -1 autocorrelation assumes that each measurement is correlated with the immediately preceding one, but not necessarily with the rest. The validity of models assuming both parametric and nonparametric distributions of the data was evaluated. It was assessed using the Quasi-likelihood under the Independence Model Criterion (QIC), and the model with the lowest QIC was selected. Pairwise comparisons were conducted using contrasts. This type of analysis imposes a penalty when making multiple comparisons. Holms' method was used to calculate the penalty.
Based on the GEE model, comparisons were made between the baseline values (at the beginning of the confinement phase) and those recorded during the confinement phase at the Base. Finally, contrasts within the GEE model were used to compare values from the winter (darkness months) and summer (daylight months) periods.
No covariates were included in the models.
Circular statistics were used to analyze the timing of the maximum and minimum HR values recorded in the 24-hour Holter ECG. Quantitative variables are expressed as means, standard deviation and 95% confidence intervals. Results are presented in hours, which are expressed in decimal format. Comparisons between groups were performed using the Watson-Williams test.
To compare winter (months of darkness) and summer (months of daylight) periods, contrasts on the adjusted GEE model including individual months were used.
The significance level was set at α = 0.05. All statistical analyses were performed using R version 4.4 (The R Foundation, Vienna), with the geepack, modelbased, performance, parameters and circular packages. (3,4,5)
Ethical considerations
The 23 individuals who joined the study signed the informed consent, which was approved by the Bioethics Committee of the Hospital Central of the Province of Mendoza. The study was conducted in accordance with the Declaration of Helsinki and amendments.
RESULTS
The 23 participants were trained males with a mean age of 34.7 ± 5.1 years (range: 27-43). Smoking was the only cardiovascular risk factor, present in only 7 subjects (30%); all were exposed to the same diet, physical demands and ambient temperature (Table 1). Measurements were taken between January 2023 and January 2024. There were no significant differences in body parameters (Table 2).
Table 1
Temperatures
| Baseline | Months of darkness | Months of daylight | |
|---|---|---|---|
| Outdoor temperature | -12.6 ± 3.34 | -22.8 ± 7.43 | -7.51 ± 6.24 |
| Indoor temperature | 21.5 ± 1.78 | 23.1 ± 0.718 | 23.8 ± 0.415 |
| Body temperature | 35.7 ± 0.819 | 35.4 ± 0.516 | 35.4 ± 0.640 |
Temperatures are expressed in degrees Celsius.
Table 2:
Body parameters
| Months of darkness | Months of daylight | ||||||
|---|---|---|---|---|---|---|---|
| Baseline (N=23) | 06-2023 (N=23) | 07-2023 (N=23) | 08-2023 (N=23) | 10-2023 (N=23) | 11-2023 (N=23) | 01-2024 (N=23) | |
| Weight (Kg) | 81.8 ± 13.9 | 81.6 ± 12.9 | 82.1 ± 13.1 | 82.0 ± 12.4 | 81.9 ± 12.0 | 81.4 ± 11.2 | 81.5 ± 11.2 |
| BMI | 27.2 ± 4.4 | 27.2 ± 4.1 | 27.1 ± 4.5 | 27.3 ± 4 | 27.3 ± 3.8 | 27.1 ± 3.6 | 27.1 ± 3.5 |
| % Body fat | 25.6 ± 7.3 | 26.3 ± 6.9 | 26.1 ± 7.6 | 26.3 ± 6.3 | 26.2 ± 6.0 | 26.1 ± 5.3 | 25.8 ± 5.4 |
| % Muscle mass | 35.9 ± 4.1 | 35.4 ± 3.9 | 35.2 ± 4.2 | 35.4 ± 3.6 | 35.5 ± 3.5 | 35.5 ± 3.0 | 35.7 ± 3.1 |
| Basal metabolic rate (Kcal/day) | 1780 ± 184 | 1770 ± 168 | 1780 ± 173 | 1780 ± 163 | 1780 ± 156 | 1770 ± 148 | 1770 ± 147 |
| Relative visceral fat (%) | 10.1 ± 4.2 | 10.2 ± 4.1 | 10.3 ± 4.3 | 10.5 ± 3.9 | 10.5 ± 3.7 | 10.3 ± 3.6 | 10.3 ± 3.5 |
| Waist (cm) | 93.3 ± 11.2 | 89.7 ± 8.4 | 89.9 ± 9.1 | 88.7 ± 8.5 | 88.8 ± 7.8 | 88.0 ± 7.1 | 88.7 ± 6.6 |
BMI, Body Mass Index.
Performance of exercise stress tests
The analysis revealed significant differences between the confinement (months of darkness and daylight) and baseline, with a decrease in HR: baseline 79.8 bpm (95% CI 75.4-85.9) vs. confinement 74.1 bpm (95% CI 71.4-78.5), p = 0.005 (Table 3).
Table 3:
Performance of the exercise stress tests
| Baseline | Months of darkness | Months of daylight | p | |
|---|---|---|---|---|
| Exercise stress test (baseline) | ||||
| SpO2* | 97.8 ± 1.4 | 97.9 ± 1.4 | 97.8 ± 1.3 | 0.324 |
| HR | 79.8 ± 12.9 | 74.3 ± 11.4 | 74.0 ± 11.3 | <0.005 |
| Systolic BP | 118 ± 11.5 | 112 ± 7.2 | 113 ± 8.8 | <0.001 |
| Diastolic BP | 76.1 ± 6.5 | 68.2 ± 8.1 | 69.9 ± 9.1 | <0.001 |
| Exercise stress test (max) | ||||
| SpO2 | 96.8 ± 1.8 | 96.2 ± 2.1 | 96.1 ± 2.4 | 0.023 |
| HR | 177 ± 10.8 | 169 ± 11.7 | 168 ± 11.0 | <0.001 |
| Systolic BP | 164 ± 15.6 | 153 ± 13.3 | 159 ± 14.3 | <0.001 |
| Diastolic BP | 88.7 ± 6.9 | 91.6 ± 6.1 | 95.4 ± 8 | <0.001 |
| Exercise stress test (recovery. 1 min) | ||||
| SpO2* | 97.7 ± 1.2 | 96.2 ± 2.1 | 96.2 ± 2.1 | 0.008 |
| HR | 147 ± 16.6 | 149 ± 13.6 | 151 ± 12.8 | |
| Systolic BP | 153 ± 19.4 | 145 ± 13.3 | 153 ± 14.9 | 0.004 |
| Diastolic BP | 78.7 ± 9.7 | 81.2 ± 8.6 | 74.9 ± 8.5 | 0.002 |
| Exercise stress test (recovery. 3 min) | ||||
| SpO2* | 98.1 ± 1.2 | 97.8 ± 1.2 | 97.3 ± 1.4 | <0.001 |
| HR | 116 ± 15.0 | 108 ± 15.4 | 107 ± 15.1 | <0.001 |
| Systolic BP | 129 ± 13.2 | 125 ± 14.0 | 125 ± 11.7 | <0.001 |
| Diastolic BP | 77.0 ± 5.6 | 74.4 ± 8.9 | 73.2 ± 8.6 | <0.005 |
| Achieved METs | 9.76 ± 1.5 | 10.0 ± 1.6 | 10.2 ± 1.42 | 0.184 |
HR, heart rate; max. maximal; METs, metabolic equivalents of O2 consumption; SpO2, peripheral oxygen saturation; BP, blood pressure.
A similar pattern was observed in systolic BP: baseline 118.26 mmHg (95% CI 114.06-122.78) vs. confinement 112.62 mmHg (95% CI 110.37-114.97), p <0.001; and in diastolic BP: baseline 76.15 mmHg. (95% CI 73.19-78.73) vs. confinement 69.84 mmHg (95% CI 66.81-70.94), p<0.001.
Similar findings were obtained for HR at maximal effort: baseline 176.91 bpm (95% CI 172.72-181.32) vs. confinement 168.76 bpm (95% CI 165.31-172.36), p<0.001; and for systolic BP at maximal effort: baseline 163.94 mmHg (95% CI 158.00-170.34) vs. confinement 155.87 mmHg (95% CI 151.56-160.45), p<0.001.
In contrast, diastolic BP at maximal effort was higher during confinement: baseline 87.85 mmHg (95% CI 85.14-90.74) vs. confinement 92.38 mmHg (95% CI 90.74-94.08), p<0.001.
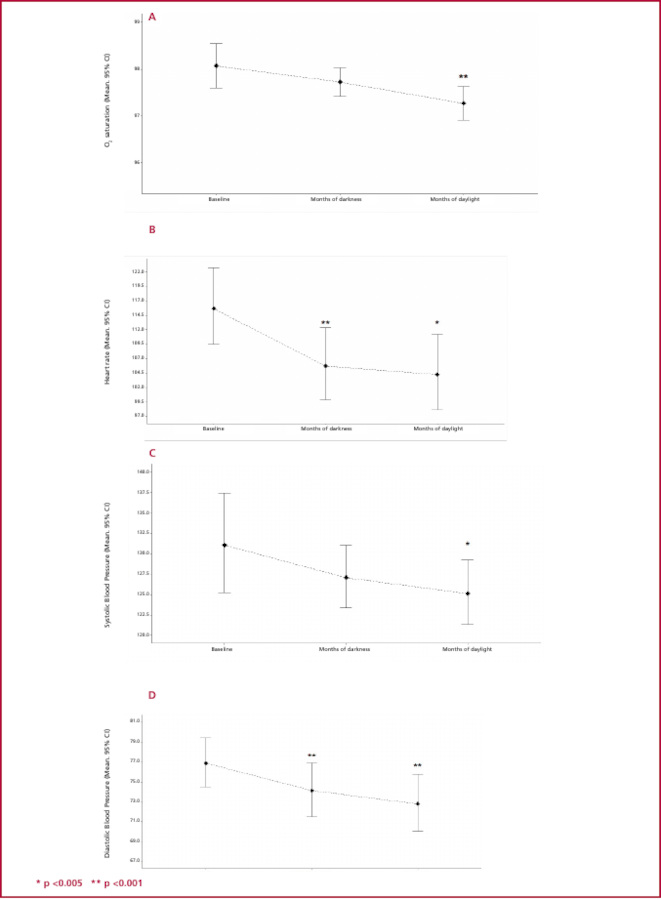
SpO2 at recovery showed a non-significant decrease: baseline 98.07% (95% CI 97.60-98.55) vs. confinement 97.49% (95% CI 97.20-97.79), p=0.003.
There were also significant differences in recovery values: HR: baseline 115.08 bpm (95% CI 108.68-122.27) vs. confinement 106.46 bpm (95% CI 100.95-112.61), p<0.001; systolic BP: baseline 128.52 mmHg (95% CI 123.54-133.93) vs. confinement 124.36 mmHg (95% CI 120.99-127.92), p=0.035; and diastolic BP: baseline 76.88 mmHg (95% CI 74.52-79.39) vs. confinement 73.48 mmHg (95% CI 71.03-76.11), p<0.001.
Figures 1, 2 and 3 show the performance of these variables during the exercise stress tests at baseline and during the months of daylight and darkness.
No differences were observed between the months of daylight and darkness, nor in the achieved METs.
Figure 1
Exercise stress test: resting parameters at baseline and during the months of darkness and daylight.
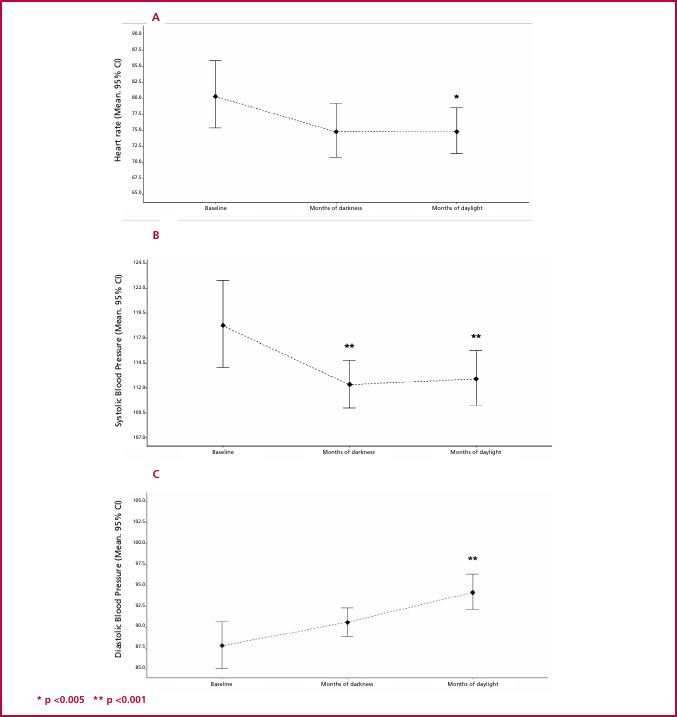
A. Heart rate; B. Systolic blood pressure; C. Diastolic blood pressure.
Figure 2
Exercise stress test: maximal effort parameters at baseline and during the months of darkness and daylight.
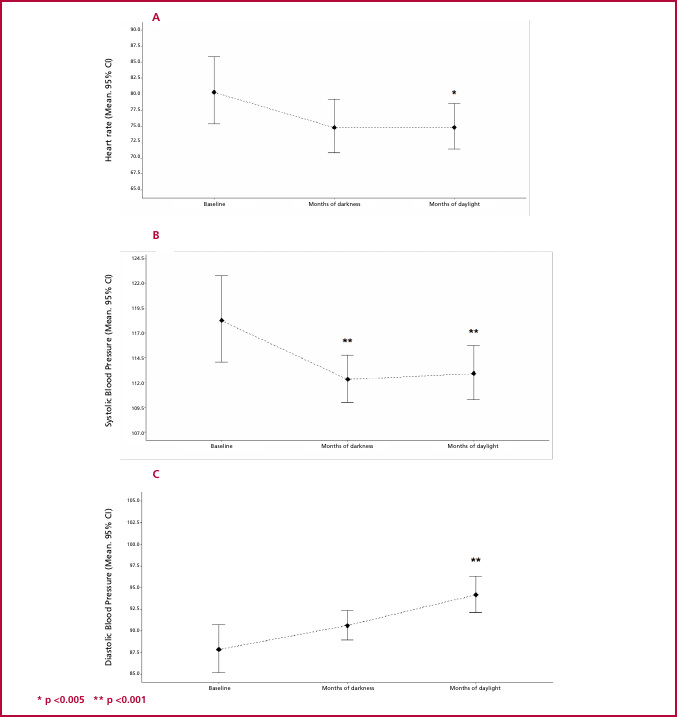
A. Heart rate; B. Systolic blood pressure; C. Diastolic blood pressure.
Analysis of Holter ECGs
A decrease in minimum HR was observed during the months of darkness and daylight compared to baseline, with no significant differences between the two timepoints (p <0.005).
The maximum HR was recorded during the outdoor work times (snow shoveling), being significantly higher during the confinement (p <0.001).
A significantly greater HR variability was observed during confinement compared to baseline (p=0.005). There was no evidence of clinically relevant arrhythmias (Table 4).
Table 4
Analysis of Holter ECGs
| Holter | Baseline | Months of darkness | Months of daylight | p |
|---|---|---|---|---|
| Minimum heart rate | 45.5 ± 10.3 | 42.0 ± 4.84 | 41.1 ± 4.17 | 0.012 |
| Time (h) | 5.56 ± 0.76 | 5.91 ± 0.79 | 5.62±0.69 | |
| Maximum heart rate | 126 ± 14.3 | 129 ± 17.0 | 131 ± 17.6 | <0.001 |
| Time (h) | 13.27 ± 1.44 | 12.84 ± 1.13 | 13.63±1.01 | |
| Differential heart rate | 80.1 ± 19.1 | 86.6 ± 17.2 | 89.5 ± 16.7 | |
| SDNN* (milliseconds) | 155.0 ± 37.7 | 164.0 ± 38.7 | 177.0 ± 33.3 | 0.003 |
SDNN, Standard Deviation of Normal-to-Normal intervals.
DISCUSSION
Most studies conducted on the White Continent have focused on sleep patterns, with limited information on the impact of complex living conditions on the cardiovascular system. (6)
Extreme environments challenge the physiological capacity of human beings to adapt to complex situations resulting from the combination of different variables, such as climate, confinement, isolation and the absence of natural light. (7)
Studying how people live under these conditions may provide valuable information, with potential benefits for health or safety. Moreover, this is one of the most accurate experimental model settings as a space analog, as it shares many specific environmental features. (8,9)
This study aimed to demonstrate physiological changes in BP and HR related to human adaptation to extreme environments, through the longitudinal collection of continuous data over a maximum period of eleven months, allowing accurate observations of changes over time.
During the confinement, a clear decrease and a marked variability in HR were observed, along with a drop in BP.
This performance reflects the activity of the autonomic nervous system on cardiac function, and suggests an increased neurovegetative pattern, predominantly vagal.
Several factors influence HR variability as well as cardiac inotropism and chronotropism in general. Such is the case of the autonomic nervous system, which regulates cardiovascular parameters, such as HR, contractile force, redistribution of blood flow to areas with greater vascular demand and short-term BP control via different sympathetic and parasympathetic receptors. (10)
It is worth exploring which physiological mechanisms might explain this performance.
Circadian rhythm disruptions
The Earth rotates on its axis, resulting in two well-defined environments: daylight and darkness. Living beings have adapted by developing specific predictive mechanisms. This gave rise to the biological rhythms that repeat every 24 hours.
Findings related to chronotype and circadian activity rhythms confirmed the role of light in synchronizing the sleep phase. A decrease in sleep duration was observed, along with a delayed chronotype and increased social jet lag during the polar night. (11,12)
In this study, the circadian cycle did not appear to influence the physiological variables analyzed, as no differences in cardiovascular behavior were detected between the periods of darkness and daylight.
Environmental pollution
The environment is a major determinant of cardiovascular health. (13) Air pollution enters the body through the alveoli and contributes to the development of cardiovascular disease by activating several mechanisms, including inflammation, endothelial dysfunction, oxidative stress, autonomic dysfunction and thrombogenicity. (14)
Chronic exposure to air pollution has been associated with increased inflammation, promoting the production of interleukin-6 (IL-6) and C-reactive protein, among other inflammatory markers associated with a higher risk of disease. (15)
Several environmental pollutants can induce autonomic dysfunction by triggering reflex arcs that alter HR and favor the onset of arrhythmias. (16) Most epidemiological studies have reported negative associations between different indices of heart rate variability and levels of fine airborne particles with a diameter of less than 2.5 micrometers (PM2.5) as well as other pollutants. (17,18)
Lead, for instance, can replace calcium in calmodulin. This mechanism has been associated with the regulation of nitric oxide synthase, which affects nitric oxide production and plays a key role in endothelial function and the inhibition of platelet aggregation.(19)
Air in Antarctica contains fewer atmospheric aerosols and presents a much more heterogeneous and diverse chemical composition compared to that of the continental regions, which may explain the lower health impact observed in the health of the study population.
Exercise effect
Physical exercise leads to a reduction in resting HR, which is also evident during physical exercise in trained individuals when performed at submaximal intensities-a phenomenon directly related to an increase in stroke volume. (20) Among the mechanisms underlying bradycardia are the regulation of the autonomic nervous system with increased vagal tone, a decrease in the intrinsic heart rate, changes in baroreceptor sensitivity, and increased systolic volume.
Regular training reduces resting sympathetic activity, lowers plasma catecholamine levels (both at rest and during submaximal exercise) and modifies renal homeostasis by decreasing renal vascular resistance-all of which contribute to BP reduction.
Exercise programs with a high dynamic component lower BP in both normotensive and hypertensive adults. This effect is more marked in hypertensive individuals, with a mean reduction of 6-7 mmHg in both systolic and diastolic blood pressure, compared to 3 mmHg reduction in normotensive individuals. (21)
The population included in our study was composed of individuals with a high level of physical training-an essential requirement for admission to the Antarctic program. Among many other reasons, candidates were selected for their strong adaptive capacity to exercise.
Furthermore, when body parameters (weight, abdominal waist circumference and body composition assessed by bioelectrical impedance) were analyzed, no differences were observed between baseline values and those recorded during the Antarctic stay. Therefore, it is unlikely that the results are influenced by the exercise effect.
Isolation and continuous stress
Antarctica is one of the most challenging environments to work in. In addition to extreme temperatures and photoperiods, Antarctic bases are remote and isolated locations usually inhabited by very few people, creating a context of limited interpersonal relationships and hostile conditions of confinement and isolation. (22,23)
During the 12-month period, the study group remained isolated, with no possibility of contact with the mainland, even in the event of an emergency. Both uncertainty and generalized fear have been described as negative factors in terms of psychological consequences. (24) Isolation lasting more than ten days has been identified as a significant risk factor for post-traumatic stress, fear, frustration, boredom and symptoms of anxiety and depression-conditions that may lead to cardiovascular alterations, such as increased HR and BP. (25)
Contrary to expectations, the mentioned cardiovascular variables tended to decrease. Positive psychological functioning was likely to act as a potential protective factor through the implementation of healthy mechanisms to cope with adversity. (26)
The military personnel voluntarily chose to participate in the expedition and undergo this experience, fully aware of the risks involved-a situation very different from imposed isolation, such as that experienced during the COVID-19 pandemic. (27)
Study Implications
The implications of this study extend to numerous areas related to healthcare, occupational health, and space exploration. Indeed, reduced HR and low BP were observed in astronauts on space shuttle missions. (28) The cardiovascular deconditioning that occurs during spaceflight includes a decrease in circulating blood volume and blood pressure-patterns very similar to our findings. (29)
In this regard, having scenarios that can rigorously replicate some of the conditions astronauts are expected to face is extremely valuable, as they offer useful contexts for advancing in space science.
New challenges in this field involve establishing permanent bases on the Moon and Mars, along with the possibility of incorporating tourist travel for untrained civilians. Therefore, the new challenges of space exploration require a deeper understanding of adaptation mechanisms in different populations. (30)
Limitations
Conclusions are limited by several factors. The sample size is small, although it worth noting that studies conducted in the Arctic or Antarctica typically involve small populations. A control group was not available, as it is almost impossible to find individuals living under the same temperature conditions and at sea level.
Another limitation is the absence of physiological parameters, such as the melatonin, cortisol and noradrenaline measurements. These assessments are planned for implementation in a future expedition.
CONCLUSION
The Belgrano II Base served as a model to explore the impact of extreme photoperiods and isolation in an environment free from atmospheric pollution on cardiovascular physiological variables. The findings suggest that under these conditions, neurovegetative activity increases. Future research is required to confirm these findings.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web).