
The immune system plays an essential role in defending the body against pathogens and cancer cells. One of the strategies that are employed in order to prevent an excessive and harmful immune response to healthy tissues is regulation through immune checkpoints. The introduction of immune checkpoint inhibitors (ICIs) has resulted in a significant therapeutic breakthrough against cancer. These drugs are monoclonal antibodies that block inhibitory receptors expressed on T cells, such as cytotoxic T lymphocyte-associated antigen 4 (CTLA-4), programmed cell death protein 1 (PD-1) or its ligand (PDL-1). As a result of this blocking, antitumor immunity is restored. (1) Immune checkpoint inhibitors have transformed the therapeutic paradigm for numerous tumors. These agents, whether administered as monotherapy or in combination with other drugs, including chemotherapy, targeted therapies, and ICI-ICI combinations, have yielded benefits that were previously unattainable for patients with advanced tumors that were resistant to other treatments.
These drugs can cause immune-mediated adverse effects in any organ of the body. Myocarditis is the most feared cardiovascular complication due to its high mortality; however, cases of non-inflammatory ventricular dysfunction, Takotsubo syndrome, pericarditis, conduction disorders and arrhythmias have also been reported. (2) A less common complication is acute myocardial infarction (AMI) due to thrombotic occlusion of an epicardial vessel (1%-3%).
We report the case of a 58-year-old female patient with a history of hypertension, morbid obesity, metabolic syndrome, nephrectomy and left adrenalectomy due to clear cell renal cell carcinoma and pulmonary metastases, who initiated a combination chemotherapy regimen with axitinib (an antiangiogenic drug) 5 mg twice daily and pembrolizumab (an anti-PD-1) every 21 days.
Five hours after receiving the seventh dose of pembrolizumab, the patients experienced a 15-minute episode of angina, which recurred at 24 and 72 hours. She presented to the cardiology clinic 12 days after the first episode, asymptomatic and with normal blood pressure, with no ST-segment abnormalities or changes relative to the electrocardiogram recorded one year earlier. On echocardiogram, the left ventricular ejection fraction was 70% and regional wall motion was normal. Hospitalization was decided because high-sensitivity troponin T level was 45.5 ng/L (VN up to 14 ng/L).
Fifteen hours after admission, the patient reported symptoms of angina and presented ST-segment elevation in the inferior and anterior leads (Figure 1 A). The coronary angiography revealed a sub-occlusion in the mid left anterior descending LAD coronary artery (Figure 2 A), and a non-significant stenosis in the proximal left circumflex artery (Figure 2 B). A drug-eluting stent was implanted in the LAD with final TIMI 3 flow (Figure 2 C). The patient's progression was free from complications and she was discharged with dual antiplatelet therapy (aspirin and clopidogrel), carvedilol, valsartan, hydrochlorothiazide, amlodipine and rosuvastatin.
Fig. 1
12-lead electrocardiograms A. First acute coronary syndrome. ST-segment elevation in leads DII, DIII, aVF, V4-V6. B. Second acute coronary syndrome. ST-segment depression in leads DI, V4-V6.
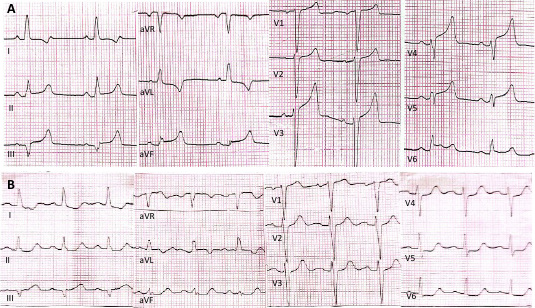
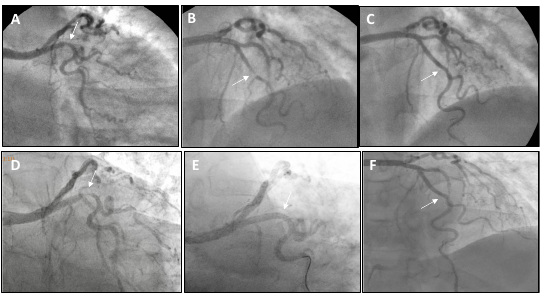
Fig.2
Top: coronary angiography during the first acute coronary syndrome. A. Non-significant stenosis in the proximal left circumflex artery. B. Sub-occlusion in the mid left anterior descending coronary artery. C. Result after percutaneous coronary in- tervention with stent implant in the left anterior descending coronary artery. Bottom: coronary angiography during the second acute coronary syndrome. D. Significant stenosis in the proximal left circumflex coronary artery. E. Result after percutaneous coronary intervention with implantation of two stents in the left circumflex coronary artery. F. The stent in the left anterior de- scending coronary artery is patent.n
The oncologists decided to discontinue axitinib therapy and continue with pembrolizumab. The eighth dose was administered 35 days after the acute coronary syndrome (ACS). Ten days later, the patient exhibited an episode of angina with ST-segment depression in DI and from V3 to V6, accompanied by increased troponin levels (Figure 1B). Coronary angiography showed a severe stenosis in the proximal left circumflex artery (Figure 2 D) and the stent of the LAD was found to be patent (Figure 2 E). Two drug-eluting stents were successfully implanted in the left circumflex artery (Figure 2 F). The patient evolved with favorable outcome and was discharged with aspirin, clopidogrel, bisoprolol, valsartan, rosuvastatin and ezetimibe.
There is evidence suggesting that ICIs can aggravate pre-existing inflammatory diseases. Atherosclerosis is a chronic vascular disease with an important inflammatory component and T cells play a key role in its initiation and progression. Immune checkpoints play a key role as negative regulators of the atherosclerotic process so their inhibition could accelerate its development. (3) Experimental studies have demonstrated that ICI treatment accelerates the progression of atherosclerosis and the formation of plaques with larger necrotic cores. A meta-analysis of 63 studies with 32 518 patients treated with ICIs showed a significant 1.51-fold increased risk of AMI and a 1.56-fold increased risk of ischemic stroke compared to the control group. (4) Atherothrombotic adverse events related to the use of ICIs occur more frequently during the first 6 months of treatment suggesting a potential destabilization of pre-existing atherosclerotic plaques.
There have been isolated case reports of an association between ICIs and ACS. Nevertheless, it is difficult to establish a cause-and-effect relationship. (5) Patients with active cancer have higher risk of developing arterial thrombosis and ischemic events particularly during the first year after diagnosis, in cases of advanced cancer and during active cancer treatment, and associated with coexistent cardiovascular risk factors, prothrombotic and inflammatory effect of the neoplasm and vascular toxic effects of cancer treatments.
In our patient, the first ACS was attributed to the use of axitinib because thromboembolic complications are more common than with ICIs. However, the rapid recurrence of ACS, involving a coronary artery that previously had a non-significant stenosis, and the temporal relationship with the administration of pembrolizumab suggest a causal link between ICI administration and ACS, a rare complication that necessitates the definitive discontinuation of treatment.
There is no evidence on the use of high doses of corticosteroids (methylprednisolone 1 g/day for 3-5 days followed by a dose reduction over 6 weeks) as recommended for other grade 3-4 adverse events (myocarditis, diarrhea or hepatitis), (6) although its empirical use has been reported in some publications on cases with ACS associated with treatment with ICIs. (5) In our case, we did not use corticosteroids.
This rare adverse effect should be suspected in cancer patients treated with ICIs.
Ethical considerations
Not applicable
Conflicts of interest
None declared. (See conflicts of interest forms on the website).