
INTRODUCTION
Heart failure (HF) is a clinical syndrome with symptoms and signs caused by a structural and/or functional cardiac abnormality, elevated natriuretic peptide levels and/or objective evidence of pulmonary or systemic congestion. (1) According to left ventricular ejection fraction (LVEF), heart failure (HF) is classified in: HF with reduced LVEF (LVEF ≤ 40%), mildly reduced LVEF (LVEF 41%-49%), and preserved LVEF (LVEF ≥ 50%). Among patients with HF with mildly reduced and preserved LVEF, patients with recovered LVEF, those with a baseline LVEF ≤ 40% and with improvement to LVEF > 40% and at least a ≥ 10% increase should be considered as a particular group. (2)
Heart failure is a global pandemic, affecting more than 64 million individuals worldwide and resulting in over 1 million hospitalizations per year in the United States and Europe. (3,4) It is estimated that the direct costs of HF account for 1-2% of the health budget in developed countries. (5) It is necessary to describe the characteristics of HF in a region from an epidemiologic and public health perspective. The PRICNASA registry, carried out in Bolivia in the city of Santa Cruz de la Sierra, observed particular characteristics in the population, such as high prevalence of Chagas disease (CD), the most common ethology of HF in the region. (6) In light of these findings, it became apparent that conducting a registry with the participation of multiple hospitals was essential to accurately reflect the regional epidemiology of HF. Santa Cruz de la Sierra, a city in the eastern plains of Bolivia, is currently the most populated city in the country, with a total population of approximately 1.6 million in 2024 and more than 3 million in the entire department of Santa Cruz. (7)
The SEPE-HF registry (Santa Cruz epidemiology and research on heart failure) is a multicenter registry, proposed by the Sociedad Cruceña de Cardiología and a group of research cardiologists, to evaluate the epidemiology of HF in Santa Cruz de la Sierra, Bolivia.
METHODS
The SEPE-HF REGISTRY is a prospective, cross-sectional, multicenter study with the participation of 7 healthcare centers in Santa Cruz de la Sierra that included tertiary health care hospitals (Hospital Obrero nº3 Caja Nacional de Salud, Caja Petrolera de Salud and Hospital San Juan de Dios), secondary health care hospitals (Hospital Municipal Francés and Hospital Universitario Hernández Vera) and private centers (Clínica Incor and Clínica Foianini). Patients hospitalized from January 2023 to April 2024 who were admitted with a diagnosis of HF due to signs and symptoms plus increased NT-proBNP (N-terminal pro-B-type natriuretic peptide) values, were included. Patients who met the inclusion criteria signed the informed consent form approved by the corresponding institutional review boards. Exclusion criteria were diagnosis of septic shock, ST-segment elevation myocardial infarction in the last 40 days, a life expectancy of less than three months, and any psychiatric disease. The aim of the registry was to determine the epidemiological characteristics, clinical presentation, evaluation, treatment and outcome of heart failure in the city of Santa Cruz de la Sierra, Bolivia.
Statistical analysis
All the statistical calculations were performed using Stata 18.0 software package. Quantitative variables are expressed as mean and standard deviation or median and interquartile range, according to their distribution. Means were compared using the t test or ANOVA, and the Wilcoxon test or Kruskal Wallis test were used to compare medians. Qualitative variables are presented as percentages and were compared using the chi-square test or Fisher's test. A p-value < 0.05 was considered statistically significant.
RESULTS
Between January 2023 and April 2024, 418 patients were included. Mean age was 67.4 ± 13.1 years and 51% were women. Mean age was 64.9 ± 13.1 years in men and 69.9 ± 12.7 years in women (p < 0.001). The baseline characteristics of the population are presented in Table 1.
Table 1
Baseline characteristics of the patients
| Characteristics | (N=418) |
|---|---|
| Age (years) | 67.4 ± 13.1 |
| Female sex | 213 (51) |
| Comorbidities | |
| HTN | 268 (64) |
| Type 2 DM | 88 (21) |
| Chronic kidney disease | 54 (13) |
| Ischemic heart disease | 50 (12) |
| COPD | 42 (10) |
| Tobacco use | 21 (5) |
| Dyslipidemia | 17 (4) |
| Previous hospitalization due to HF | 109 (26) |
| Functional class (NYHA) | |
| II | 62 (14.9) |
| III | 223 (53.3) |
| IV | 133 (31.8) |
| Signs and symptoms | |
| Lower limb edema | 309 (73.9) |
| Cardiac enlargement | 233 (55.7) |
| Dyspnea | 327 (78.2) |
| Crackles | 279 (66.6) |
| APE | 22 (5.2) |
| Jugular venous distension | 244 (58.3) |
| Pleural effusion | 87 (21.2) |
| Nicturia | 84 (20.0) |
| Nocturnal cough | 77 (18.4) |
| Tachycardia | 66 (15.7) |
| Heart rate (bpm) | 85 (± 26.5) |
| SBP (mm Hg) | 126.7 ± 29.6 |
| DBP (mm Hg) | 75.8 ± 16.2 |
| Oxygen saturation (%) | 94 ± 4.7 |
| Electrocardiogram | |
| Atrial fibrillation | 124 (29.7) |
| Pacemaker rhythm | 44 (10.5) |
| RBBB | 53 (12.7) |
| LBBB | 47 (11.2) |
| LAH | 54 (12.9) |
| Laboratory | |
| Creatinine (mg/dL) | 1.29 (1-1.6) |
| NT-proBNP (pg/mL) | 700 (200-3142) |
Baseline characteristics of the patients included in the registry.
APE: acute pulmonary edema; COPD: chronic obstructive pulmonary disease; DBP: diastolic blood pressure; DM: diabetes mellitus; HF: heart failure; HTN: hypertension; LAH: left anterior hemiblock; LBBB: left bundle branch block; NT-proBNP: N-terminal pro-B-type natriuretic peptide; NYHA: New York Heart Association; RBBB: right bundle branch block; SBP: systolic blood pressure.
Qualitative variables are presented as frequency and percentage, and quantitative variables are expressed as mean and standard deviation or median and interquartile range.
Mean heart rate on admission was 84 ± 26.5 beats per minute, systolic blood pressure was 126.6 ± 29.6 mm Hg and diastolic blood pressure was 75.3 ± 16.2 mm Hg. Most patients were in functional class III and IV. The predominant signs and symptoms were dyspnea, jugular venous distension, bibasilar crackles and bilateral lower extremity edema. The admission laboratory showed slightly impaired renal function and a median NT-proBNP of 700 pg./mL (200-3142). The ECG showed sinus rhythm in 57.8% of patients and atrial fibrillation in 29.8%. Average QRS complex width was 110 ms.
Seventy-five percent of patients underwent transthoracic echocardiography; 51% presented LVEF ≤ 40%. Among patients with LVEF ≤ 40%, 62.4% were male versus 43% in those with higher LVEF; this difference was statistically significant (p < 0.001). The causes of HF decompensation included infection in 33%, treatment discontinuation in 31.3%, hypertensive emergency in 10.5%, cardiac arrhythmias in 7.1% and acute coronary syndrome in 4%.
The primary etiology of HF was CD (36.7%), followed by hypertension (29.9%), ischemic heart disease (19.2%), severe mitral valve disease (16%), arrhythmia (8.6%) and severe aortic valve disease (6.9%). Table 2 presents the prevalent etiologies according to age range (< 50 years, 50-70 years, > 70 years).
Table 2
Etiology of heart failure
| Etiology | < 50 years | 50-70 years | > 75 years | p |
|---|---|---|---|---|
| n = 42 | n =243 | n = 133 | ||
| Ischemic heart disease | 4 (10.2) | 43 (17.8) | 25 (19.2) | 0.400 |
| Severe mitral valve disease | 13 (33.3) | 56 (23.2) | 9 (9.9) | 0.001 |
| Severe aortic valve disease | 3 (7.6) | 24 (9.9) | 8 (6.1) | 0.490 |
| Hypertrophic cardiomyopathy | 0 (0) | 3 (1.2) | 7 (5.3) | 0.050 |
| Idiopathic dilated cardiomyopathy | 3 (7.6) | 2 (0.8) | 3 (2.3) | 0.020 |
| HTN | 4 (10.2) | 78 (32.3) | 47 (36.1) | 0.005 |
| Induced by arrhythmias | 1 (2.5) | 27 (11.2) | 16 (12.3) | 0.190 |
| Chagas cardiomyopathy | 11 (28.2) | 86 (35.6) | 58 (43) | 0.100 |
| Congenital heart disease | 5 (12.8) | 1 (0.4) | 0 (0) | 1.000 |
Etiology of heart failure by age group
HF: heart failure; HTN: hypertension.
Qualitative variables are presented as frequency tables and percentages.
A comparison of the characteristics of patients with CD and those without CD revealed that patients with CD tended to be older, had a lower prevalence of hypertension, and higher prevalence of right bundle branch block, atrial fibrillation (AF), and pacemaker rhythm. Patients with CD had higher prevalence of reduced LVEF. Prior use of diuretics, mineralocorticoid receptor antagonists and gliflozins was greater in these patients but the use of renin angiotensin system inhibitors and angiotensin II receptor blockers was lower. Table 3 shows the characteristics of both groups.
Table 3
Comparison of patients with and without Chagas diseas
| With Chagas | Without Chagas | p | |
|---|---|---|---|
| 153 (36.6%) | 265 (63.4%) | ||
| Age, years | 68.8 ± 11.9 | 66.5 ± 13.7 | 0.083 |
| Female sex | 72 (47.1) | 131 (49.4) | 0.714 |
| HTN | 76 (49.6) | 186 (70.1) | 0.001 |
| DM | 27 (17.6) | 58 (21.8) | 0.362 |
| Tobacco use | 8 (5.2) | 14 (5.2) | 1.000 |
| Stroke | 8 (5.2) | 8 (3) | 0.384 |
| Ischemic heart disease | 5 (3.2) | 44 (16.6) | 0.001 |
| Pacemaker | 40 (26.1) | 3 (3.7) | 0.001 |
| CRT | 3 (1.9) | 1 (0.3) | 0.280 |
| ICD | 1 (0.6) | 1 (0.3) | 1.000 |
| Sinus rhythm | 61 (39.8) | 176 (76.4) | 0.001 |
| AF/atrial flutter | 58 (37.9) | 61 (23) | 0.001 |
| Pacemaker rhythm | 34 (22.2) | 10 (3.7) | 0.001 |
| RBBB | 27 (17.6) | 24 (9) | 0.015 |
| LBBB | 19 (12.4) | 28 (10.5) | 0.676 |
| Creatinine (mg/dL) | 1.30 (0.91-1.62) | 1.29 (1.02-1.65) | 0.155 |
| NT-proBNP | 500 (107-2555) | 805 (237-3612) | 0.162 |
| RASi | 92 (60.1) | 209 (78.8) | 0.001 |
| BB | 77 (50.3) | 132 (49.8) | 1.000 |
| MRA | 90 (58.8) | 132 (49.8) | 0.093 |
| SGLT2i | 78 (50.9) | 80 (30.1) | 0.001 |
| Diuretics | 99 (64.7) | 141 (53.2) | 0.028 |
| LVEF < 40% | 91 (59.4) | 72 (27.1) | 0.001 |
| LVEF 41-49% | 17 (11.1) | 41 (12) | 0.273 |
| LVEF >50% | 16 (10.4) | 79 (29.8) | 0.001 |
| Length of stay (days) | 6 (3-12) | 7 (2-12) | 0.982 |
| CV mortality | 13 (8.4) | 14 (5.2) | 0.279 |
Comparison of HF patients' characteristics according to the presence or absence of Chagas disease
AF: atrial fibrillation; BB: beta-blockers; CAF: chronic atrial fibrillation; CRT: cardiac resynchronization therapy; DM: diabetes mellitus; HTN: hypertension; ICD: implantable cardioverter defibrillator; LBBB: left bundle branch block; LVEF: left ventricular ejection fraction; MRA: mineralocorticoid receptor antagonist; NT-proBNP: N-terminal pro-B-type natriuretic peptide; PM: pacemaker; RASi: renin-angiotensin system inhibitors; RBBB: right bundle branch block; SGLT2i: sodium-glucose co-transporter 2 inhibitor.
Qualitative variables are presented as frequency and percentage, and quantitative variables as mean and standard deviation or median and interquartile range.
Treatment in the acute setting included the administration of intravenous bolus of loop diuretics in 90% of cases with an average dose of 68 mg/day. The use of noradrenaline was 9.5%, dobutamine 8.8%, nitroglycerin 5.5%, and dopamine 2.3%. Cardiovascular mortality was 5.5% (7.3% in patients with reduced LVEF). In these patients the incidence of cardiogenic shock was 11.5%. Cardiovascular mortality was not significantly higher in patients with CD.
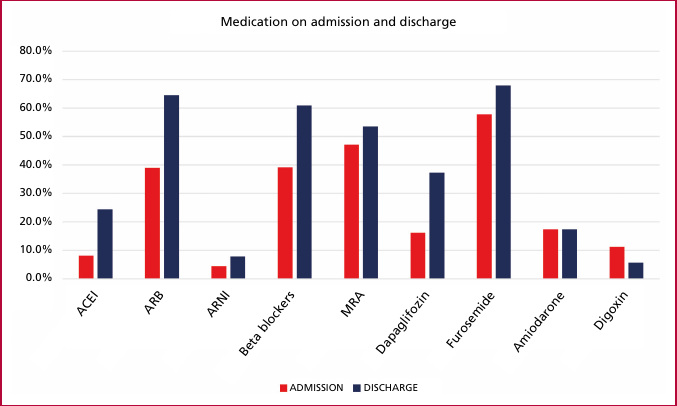
The mean length of hospital stay was 14 days for all the patients in the registry. Heart failure treatment was optimized at hospital discharge, with indications for angiotensin-converting enzyme (ACE) inhibitors increasing from 8% to 28%, angiotensin II receptor blockers from 39% to 68%, sacubitril-valsartan from 4% to 15.8%, beta-blockers from 39% to 53%, mineralocorticoid receptor antagonists from 47% to 67%, and dapagliflozin from 16% to 58% (Figure 1).
DISCUSSION
The SEPE-HF registry included 418 patients in the city of Santa Cruz de la Sierra, Bolivia. We observed a heterogeneous population with advanced mean age and predominantly female, consistent with other cohorts. (5,8) The baseline characteristics of the patients and their cardiovascular risk factors reflect similar characteristics to the population of an important and recent registry such as the Argentine Registry of Heart Failure ARGEN-IC. (9) However, in our population the prevalence of tobacco use was much lower, and the history of CD was higher. The most common etiology of HF in various publications is mainly ischemic heart disease, but was only 19.2% in our registry, a low percentage compared to the ARGEN-IC registry where it was 26%. (9) In the population <50 years, the main causes were rheumatic heart disease and congenital heart disease. We should highlight that CD is the most common etiology in our registry (36.7%), which is high compared to other registries in countries where CD is present. The PRICNASA registry had already demonstrated a high prevalence of patients with CD in our region, confirmed by the SEPE-HF registry. (6) Chagas disease affects about 10-12 million people worldwide. (10) In the natural history of CD, cardiac impairment progressively develops 20-30 years after the initial infection. (11) In Bolivia, CD has been historically endemic in approximately 60% of the national territory. In 1999, the domestic infestation rate in Bolivia was 55% and decreased to 1.5% in recent years, while the rate of houses intra-domestically infested decreased from 24.2% to 0.4% in the same years. (12) Despite the high burden of morbidity and mortality associated with CD and the high cost to national healthcare systems, 70-90% of people with the disease are unaware of their diagnosis and only 1% receive adequate etiologic treatment. (13,14,15) However, once the disease progresses to more advanced clinical stages with severe cardiac involvement, etiologic treatment does not appear to provide clinical benefit. (16,17,18)
Because of the complexity of the pathophysiology and clinical characteristics of CD, this group of patients is not represented in any of the HF studies. There is little evidence on the management of these patients. It is imperative that registries and studies are conducted that continue to evaluate the outcome of HF in patients with CD, including treatment. The PARACHUTE HF trial will evaluate the effect of sacubitril-valsartan vs. angiotensin-converting enzyme inhibitors (ACEI) in patients with LVEF < 40% and CD, to provide randomized and contemporary evidence to guide medical decisions in these patients. (19)
Twenty-six percent of patients in the SEPE-HF registry had previous hospitalization for HF. About 84.9% had FC III-IV dyspnea. The clinical profile on admission was similar to the one observed in the ARGEN-IC registry. (9) Echocardiograms were conducted in 75% of patients. Not all patients were tested, perhaps due to lack of resources. In the ARGEN-IC registry, 90% of patients underwent echocardiography, with an average LVEF of 41%. Forty-nine percent of patients had reduced LVEF, a figure similar to the one in our registry. (9)
The low use of intravenous vasodilators was similar to that observed in the rest of the registries. Pharmacological treatment could be optimized at hospital discharge, in line with the scientific evidence available. Although treatment was optimized, it is imperative to closely monitor these patients to ensure continuous optimization of the mainstays of HF treatment. The SEPE-HF registry showed a deficit of influenza vaccination in our patients, suggesting that we should be more aware of the need for protocolisation.
In-hospital mortality (5.5%) is in the range of that observed in other registries: 7.9% in ARGEN-IC, (9) 4% in ADHERE, (8) and 6.7% in Euro Heart Failure Survey II. (20) This cohort provides us with the opportunity to obtain current information on the HF population in Santa Cruz de la Sierra, Bolivia, and to design new strategies and approaches for our patients hospitalized for HF.
CONCLUSION
The SEPE-HF registry is a representation of HF in our population. We observed similarities in terms of our incidence in many epidemiological factors, comorbidities, and clinical profile with the ARGEN-IC registry. Chagas disease remains a significant etiology of HF in our population, a factor that should be considered in future studies, strategies, and health policies. The mortality rate in our registry is consistent with global standards.
Conflicts of interests
None declared. (See authors' conflict of interests forms on the web).