
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a genetic, structural heart disease charac- terized by the progressive atrophy of the ventricular myocardium and replacement by fibro-fatty tissue. It has been widely described that ARVC typically pro- gresses from the epicardium to the endocardium; therefore, the results of ablation via the endocardial approach are limited. Some studies involving a small number of patients suggest that a combined endo-epi- cardial approach yields better results. We present the case of a 38-year-old male patient with ARVC who was referred to our center due to an electrical storm and was treated using the endo-epicardial approach.
The patient was diagnosed with ARVC at age 18, when cardiac magnetic resonance imaging revealed in- ferolateral gadolinium enhancement in the right ven- tricle (RV). An implantable cardioverter-defibrillator (ICD) was implanted in 2014 for secondary prevention of sudden death. He was referred to our department due to multiple episodes of ventricular tachycardia (VT) with appropriate ICD shocks (3 episodes within the last 24 hours). Doppler echocardiography showed RV dilatation with preserved systolic function; the RV diameter was 45 mm in the 4-chamber view. Tricuspid annulus plane systolic excursion (TAPSE) was 24 mm and peak systolic velocity at the lateral tricuspid an- nulus by pulsed wave tissue Doppler imaging (S-wave TDI) was 0.08 m/s. Right ventricular fractional short- ening was 38%. We decided to perform endo-epicardial catheter ablation.
Under general anesthesia, programmed ventricu- lar stimulation was performed from the RV apex (S1S1-S2: 600-320 ms) inducing sustained VT with complete left bundle branch block morphology, inferior axis and R wave transition in V4, and absence of hemodynamic instability. The procedure continued with activation mapping during VT and scar mapping of the RV outflow tract, with the area of the greatest interest in the anterior region of the RV (precocity of 25 ms), topo-stimulation: 94%. The next step was the epicardial approach.
The procedure began with the instillation of lido- caine, followed by the needle-in-needle technique to access the pericardium. A 18G external needle was inserted below the xiphoid process. After inserting the 18 needle, a 21 micropuncture needle was intro- duced and advanced until the heartbeat was felt, indi- cating entry into the pericardial space. Radio-opaque contrast was injected to confirm optimal positioning. Then, a 0.018-inch guidewire was advanced through the micropuncture needle. After verifying the correct positioning of the needle within the pericardial sac, the needle was removed. A flexible introducer was ad- vanced and the 0.018-inch guidewire was exchanged for a 0.032-inch guidewire. A standard 8F introducer was advanced over this guidewire.
The Pentaray mapping catheter and the con- tact force sensing ablation catheter were advanced through the 8 Fr introducer. A non-fluoroscopic-based three-dimensional navigation system was used for epicardial anatomical reconstruction and to create an activation map of VT with evidence of its entire circuit and of mesodiastolic potentials in the anterior region of the RV. This resulted in the cessation of VT.
Voltage map and isochronal late activation map- ping (ILAM) with deceleration zones were created during sinus rhythm. There was evidence of greater scar extension in this area, as well as late potentials in the anterior region of the RV, in coincidence with the activation map. Topo-stimulation was performed with 98% agreement in the same area. A total of 35 applications of radiofrequency energy (25 W) were delivered using an external contact force sensing catheter with an irrigated tip until the diastolic potentials disappeared during sinus rhythm. Endocardial applications were complemented from the anterior region of the RV (35 W). At the end of the procedure, programmed ventricular stimulation was performed (S1-S1-S2: 500-280-280 ms) up to the ventricular refractory pe- riod, without inducing VT. A pericardial drain was left in place for 48 hours, and no complications devel- oped. After a 10-month follow-up period, the patient remained free of arrhythmias.
Fig. 1
A. Endocardial right ventricular (RV) activation mapping. B. Ventricular tachycardia. C. Voltage map. D. Epicardial approach with guidewire placed in the pericardium, ablation catheter in the right ventricular outflow tract (RVOT) and intracardiac ultra- sound probe in the right atrium. E. ECG showing sinus rhythm with inverted T-waves in the right precordial leads. F. Catheter in the pericardium for mapping points in high-density mapping, ablation catheter in the RVOT, ultrasound probe. G. Applications of radiofrequency energy from the endocardial surface of the RV.
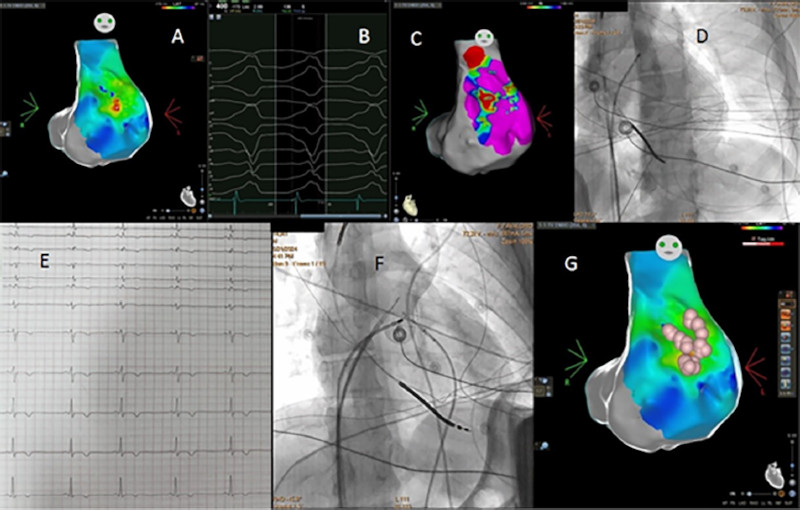
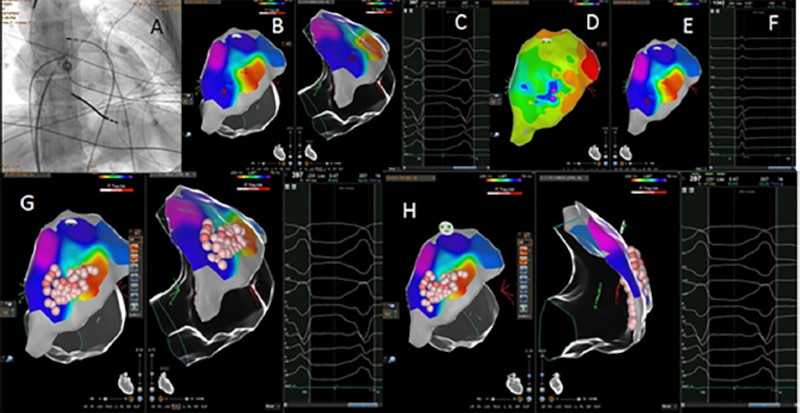
Fig. 2
A. Fluoroscopy showing contact force sensing catheter in the pericardium. B. Activation map from the pericardium. C. Ventricular tachycardia. D and E. Isochronal late activation mapping (ILAM) with deceleration zones in coincidence with the activation map during tachycardia. F. Sinus rhythm with late potentials. G. Applications of radiofrequency (RF) energy from the epicardium. H. G. Applications of RF energy from the endocardium and epicardium.
The patient's progress indicates that voltage and deceleration maps in sinus rhythm are a useful tool that correlates with the activation map during tach- ycardia, and that VT ablation with a first-line endo- epicardial approach provides promising results in pa- tients with ARVC.
Ethical considerations
Not applicable
Conflicts of interest
None declared. (See conflicts of interest forms on the website).