
INTRODUCTION
Patients with type 2 diabetes mellitus (DM2) are at a higher risk for cardiovascular disease than other population groups with similar characteristics without DM2. (1,2) The administration of lipid-lowering medications, aimed at reducing plasma levels of low-density lipoprotein cholesterol (LDL-C), has been demonstrated to result in a reduction in major cardiovascular events in various clinical trials, irrespective of the presence of DM2. However, the risk of developing new cardiovascular events persists even when LDL-C levels drop below 55 mg/dL. (3,4) The presence of moderate hypertriglyceridemia is a common characteristic of patients with DM2. (5) The use of icosapent ethyl (IPE) in patients with atherosclerotic cardiovascular disease (ASCVD) or DM2 associated with another cardiovascular risk factor and elevated triglycerides was associated with a 25% reduction in the risk of major cardiovascular events in the REDUCE- IT (Reduction of Cardiovascular Events with Icosapent Ethyl-Intervention Trial) study. (6) These results led to the incorporation of this new therapeutic option in clinical practice guidelines to reduce residual risk in this population. (7,8) Although this treatment has recently been approved in Argentina, the proportion of patients with DM2 who could be considered candidates to receive it is unknown. The aim of this study is to evaluate the eligibility of patients with DM2 who could benefit from treatment with icosapent ethyl (IPE) in terms of cardiovascular risk reduction.
METHODS
We conducted a descriptive and retrospective study. Patients with DM2 who were included in the registry of the Council on Cardiometabolism of the Argentine Society of Cardiology between May and July 2019 were included. Patients hospitalized were excluded from the study, as well as those with type 1 diabetes, secondary DM, pregnancy and those who refused to be included in the protocol. The clinical characteristics and the laboratory findings were evaluated. Patients were considered eligible for IPE if they were between 40 and 75 years of age, had a history of ASCVD or 2 associated risk factors, were receiving statin therapy, and had LDL-C levels
< 100 mg/dL and TG levels between 150 and 499 mg/dL. Eligibility for IPE was assessed in the total population, in the population of patients with ASCVD (history of coronary artery disease, cerebrovascular disease, or peripheral vascular disease), and in those without ASCVD. The study was conducted following the recommendations of the Declaration of Helsinki revised in 2003. (9) The participation was voluntary and all the patients signed an informed consent form to be included in the study. Qualitative variables are presented as frequency and percentage, and quantitative variables as mean and standard deviation (SD). Statistical significance was considered with a 2-tailed p-value < 0.05.
RESULTS
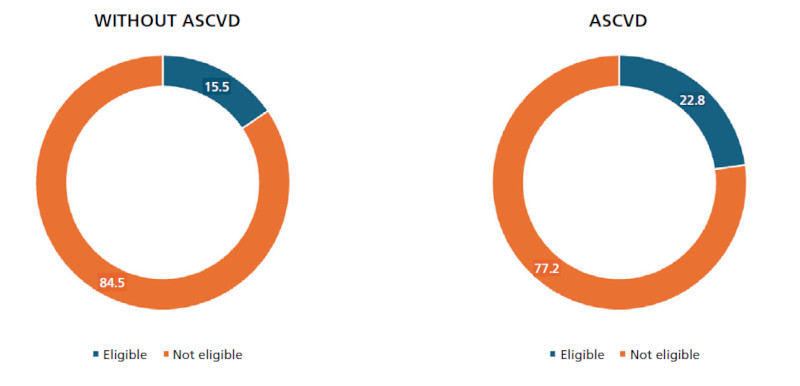
A total of 694 patients included in the registry of Cardiometabolism of the Argentine Society of Cardiology were evaluated. Of these, 601 had a complete lipid profile, 51.7% (311 patients) had ASCVD and 48.3% (290 patients) were in primary prevention. Mean age was 67.2 ± 9.3 years; 60.1% were male and 91.7% had hypertension. The mean body mass index was 32 kg/ m2. Mean glycated hemoglobin was 7.3 %, mean LDL- C was 95 mg/dL, mean TG was 166.5 mg/dL and mean glomerular filtration rate was 78.6 mL/min/1.73m2; 72.4% were receiving statins, and 7.1% were receiving ezetimibe. The differences between patients with and without ASCVD are presented in Table 1. Patients with ASCVD were predominantly male, older and were using statins and ezetimibe, which explains the lower total and LDL cholesterol values. After applying the eligibility criteria for IPE, 19.3% of the patients were deemed eligible (Figure 1). When these patients were divided according to the history or absence of ACVD, 22.8% (71 patients) in secondary prevention and 15.5% (45 patients) in primary prevention met criteria for receiving IPE (OR 1.61, 95% CI 1.04-2.49; p= 0.029). (Figure 2).
Table 1
Baseline characteristics
| Without ASCVD | With ASCVD | Total | p* | |
|---|---|---|---|---|
| (n = 290) | (n = 311) | (n = 601) | ||
| Age, years (mean ± SD) | 63 ± 9.6 | 67 ± 9.7 | 65 ± 9.8 | < 0.001 |
| Male sex, (%) | 45 | 69 | 57.6 | < 0.001 |
| HTN (%) | 90 | 93 | 91.7 | 0.241 |
| BMI (mean ± SD) | 32.5 ± 5.9 | 31.5 ± 6.1 | 32 ± 6 | 0.041 |
| DM2 diagnosis > 10 years (%) | 34.5 | 43 | 38.9 | 0.036 |
| HbA1c,% (mean ± SD) | 7.3 ± 1.7 | 7.2 ± 1.4 | 7.3 ± 1.6 | 0.430 |
| Total cholesterol, mg/dL (mean ± SD) | 181 ± 45.8 | 159 ± 43 | 170 ± 45.7 | < 0.001 |
| HDL-cholesterol, mg/dL (mean ± SD) | 45 ± 11.7 | 44 ± 24.13 | 44.5 ± 26 | 0.523 |
| LDL-cholesterol, mg/dL (mean ± SD) | 105 ± 40 | 85 ± 36.2 | 95 ± 39.3 | < 0.001 |
| Triglycerides, mg/dL (mean ± SD) | 173 ± 103.6 | 160 ± 79.8 | 166.5 ± 92.1 | 0.084 |
| GFR, mL/min/1.73m2 (mean ± SD) | 84 ± 20 | 73 ± 21.6 | 78.5 ± 21 | < 0.001 |
| Statins (%) | 62.4 | 81.6 | 72.4 | < 0.001 |
| Ezetimibe (%) | 4.5 | 9.6 | 7.1 | 0.017 |
| Insulin (%) | 19 | 25.6 | 22.5 | 0.062 |
| GLP-1 RA (%) | 2.4 | 3.5 | 5.9 | 0.478 |
| SGLT2i (%) | 6.2 | 12.8 | 20 | 0.006 |
*: without ACVD vs. with ACVD
ASCVD: atherosclerotic cardiovascular disease; BMI: body mass index; DM2: type 2 diabetes mellitus; GFR: glomerular filtration rate; GLP-1 RA: glucagon-like peptide 1 receptor agonists; HbA1c: glycated hemoglobin; HDL: high-density lipoprotein; HTN: hypertension; LDL: low-density lipo- protein; SD: standard deviation; SGLT2i: sodium-glucose co-transporter 2 inhibitors

DISCUSSION
This study showed that, in a cohort of patients with DM2 with high and very high cardiovascular risk, one out of five patients met the criteria for eligibility to receive IPE. Rawshani et al. showed a reduction in both death from cardiovascular disease and death from coronary artery disease and hospitalizations for cardiovascular disease over the last 20 years, with a smaller reduction in patients with DM2. This finding suggests the presence of a notable increase in residual risk within this patient population. (10) The emergence of novel pharmacological groups that have shown a reduction in major cardiovascular events, risk of hospitalization for heart failure and even cardiovascular mortality in some patient subgroups across various clinical studies, shows that this residual risk exists and that it can be reduced through the incorporation of novel therapeutic options. (11,12) However, beyond these interventions, the high incidence of cardiovascular events observed, especially in studies that included patients with DM2 at very high cardiovascular risk, makes it necessary to address other variables in order to achieve a greater reduction. Despite the above, the use of drugs with proven cardiovascular benefits remains suboptimal, (13) if we consider that only 25.9% of patients in this registry received medications with documented cardiovascular benefits. Hypertriglyceridemia and remnant cholesterol emerge as therapeutic targets of interest, particularly in patients with DM2 who have a higher prevalence of elevated triglyceride levels than other patient subgroups. Omega-3 fatty acids are among the drugs evaluated in patients with these characteristics. The JELIS (Japan EPA Lipid Interventional Study) study, conducted in Japan, included patients with total cholesterol levels ≥ 250 mg/ dL. Treatment with 1,800 mg of eicosapentaenoic acid (EPA) combined with statins reduced the risk of ma jor cardiovascular events by 19%, compared to treatment with statins alone. (14) In the same line, the REDUCE-IT study compared the use of 4 g/day of EPA associated with statins with or without ezetimibe ver sus treatment with statins with or without ezetimibe. Once again, there was a reduction in major cardiovascular events, this time by 25%, as well as a reduction in most of the evaluated secondary endpoints. (6) It is important to highlight that in this study 57.8% of the patients had DM2. Subsequently, the EVAPORATE study demonstrated that the use of 4 g/day of IPE was associated with changes consistent with atheroma plaque regression. (15) The exact mechanisms by which this benefit occurs are still under discussion. However, it is suggested that the risk reduction with IPE treatment exceeds the observed reduction in TG levels. (16,17) Based on these results, clinical practice guidelines have recommended considering the use of IPE for patients with DM2 or ASCVD who are receiving statins and have TG between 150 and 499 mg/dL, in order to reduce cardiovascular risk.
One limitation of our study is that eligibility was defined based on the treatment received by the patients, without specifying the dose of statins used or the proportion of patients receiving other drugs such as fibrates for the treatment of hypertriglyceridemia. We must also consider the fact that 70% of patients were receiving statins, which can lead to an underestimation or overestimation of the actual triglyceride value and thus influence eligibility. Likewise, the population evaluated may not represent the total number of patients with DM2 but rather the one evaluated in a cardiology office.
In conclusion, in a real-world population of patients with DM2 who are monitored by cardiologists in Argentina, 1 out of 5 patients is eligible for treatment with IPE, which has the potential to reduce cardiovascular events.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web).