
INTRODUCTION
Fontan-Kreutzer surgery (FS) for patients with univentricular physiology consists in the generation of a "serial" circuit, with a single systemic ventricle as a pulsatile pump that maintains cardiac output, and directly connects the systemic venous return to the pulmonary artery without interposition of a functional subpulmonary ventricle. (1,2) Over time, this fragile hemodynamic model, characterized by elevated central venous pressure and chronic low output state, has deleterious effects on multiple organs. (3,4)
About 3% to 20% of patients will develop protein-losing enteropathy (PLE), defined as a severe loss of albumin and other proteins in the intestinal lumen, with a high impact on survival. It is suspected from the patient's history and physical examination, and is confirmed by the presence of hypoalbuminemia and elevated level of alpha 1 antitrypsin (AT) in the stools. (5) Survival at five years from diagnosis was initially described as low as 50%; however, with recent advances in early diagnosis and new treatments, survival at 5 and 10 years is currently 88% and 72%, respectively. (6,7,8)
The pathophysiology of PLE, although extensively studied, remains controversial and is not fully elucidated. Undoubtedly, the chronic increase in systemic venous pressure sustained over time is a determining factor, but it alone does not fully explain all the phenomena leading to protein leakage into the intestinal lumen. Two key observations have prompted the search for new answers: first, although all patients with Fontan-Kreutzer circulation have elevated systemic venous pressure, not all develop this complication; second, published studies have not shown a direct relationship between the value of central venous pressure and the severity of enteropathy. A better correlation has been found in those patients who, in addition to increased venous pressure, present a clearly decreased cardiac output, establishing increased peripheral resistance specially involving "non-vital" organs, such as the gastrointestinal system. In patients with PLE, diastolic flow in the mesenteric artery is markedly decreased or even absent. (9,10) This "compensatory" mechanism results in a significant reduction of perfusion flow and, at the cellular level, apoptosis, which compromises the integrity of the intestinal barrier and facilitates protein loss. (11) Protein-losing enteropathy occurs in gastrointestinal or systemic inflammatory diseases (such as Crohn's disease or systemic lupus erythematosus) and responds favorably to corticosteroids, further suggesting an inflammatory component in its pathophysiology. (12,13) Similarly, treatment with heparin has shown some effectiveness, acting by its chemical structure as a barrier for the passage of proteins into the enterocyte, given that both are negatively charged molecules. (14) Finally, the reduction of oncotic pressure due to protein loss causes generalized edema, even in the intestinal wall, which further hinders the adequate absorption of nutrients, creating a vicious circle that aggravates the already existing clinical condition.
In recent years and with the advent of new imaging modalities, such as nuclear magnetic resonance lymphography or catheterization, pathological dilatation of the hepatoduodenal lymphatic ducts, lymphangiectasias, collateralization of the lymphatic system and even the presence of retrograde lymphatic flow into cavities of lower pressure, such as the bronchi or intestine, have also been demonstrated
These findings suggest the existence of a congenital defect present in the lymphatic system of affected patients, which acts as another predisposing factor for the development of this entity. (15,16,17,18,19,20) Based on these observations, the technique of lymphatic duct embolization has been proposed as a novel specific therapeutic target with encouraging results, initially described by Itkin et al. (19,20,21)
OBJECTIVE
The aim of this study was to evaluate the feasibility, complications and clinical-analytical outcome of selective hepatoduodenal lymphatic embolization (SHDLE) in patients with Fontan-Kreutzer circulation and PLE.
METHODS
A retrospective review was carried out of the clinical history of patients with FS who evolved with PLE and underwent an SHDLE procedure. We defined PLE as the presence of compatible signs and symptoms (soft tissue edema, diarrhea and ascites) accompanied by decreased serum albumin levels (< 3.2 g/dL) and elevated alpha 1 AT clearance (Cl) in the stools (Cl 24 hs > 20 mL). The lymphography and percutaneous embolization technique was performed as described by Itkin et al. (19) We evaluated serum albumin levels 10 days and 4 months after the procedure, and at the last control of each patient.
RESULTS
Five patients (P1 to P5) with FS performed at a median age of 4 years (range 3.5-4.3) were included in this study. Three patients developed the characteristic clinical condition of PLE, and in two patients the presentation was subclinical, both by routine laboratory findings: one presented with isolated hypoalbuminemia, and the other with increased alpha 1 AT clearance in the stools and normal protein and albumin. The latter case was interpreted as incipient PLE. The patients included presented the diagnosis of PLE at a median time of 7 years (range 2.3-15.3) from the performance of the FS.
Patient characteristics are listed in Table 1.
Table 1
Baseline characteristics
| Pt | Sex | Age (years) | Type of SV | Surgery | FS (age in years) | PLE after Fontan (years) | SO2 (%) | CVP (mmHg) | Time with PLE symptoms | Treatment for PLE |
|---|---|---|---|---|---|---|---|---|---|---|
| P1 | Fem | 8 | HLVS | ECT (F) F permeable | 4 | 2.5 | 88 | 19 | 4 months | aspirin, sildenafil, bosentan, enalapril, spironolactone, carvedilol, furosemide, anticoagulation. budesonide, albumin, diet |
| P2 | Male | 21 | DILV criss cross type | ECT (F) F closed by catheterization | 4 | 7 | 96 | 15 | 7 years | aspirin, sildenafil, bosentan, enalapril, eplerenone, atenolol, furosemide, anticoagulation, budesonide, albumin, diet |
| P3 | Fem | 20 | DILV criss cross type | ECT (NF) | 3.5 | 15.3 | 96 | 12 | subclinical | aspirin, anticoagulation, sildenafil, furosemide, spironolactone, diet |
| P4 | Male | 7 | HLVS | ECT (F) Spontaneous closed F (later required surgical re F) | 4.3 | 2.3 | 96 | 19 | 2 years | aspirin, sildenafil, enalapril, spironolactone, furosemide, anticoagulation, budesonide, albumin, diet. LPB angioplasty - Septectomy and fenestration of the system. |
| P5 | Fem | 19 | HLVS ¿ | ECT (F) F closed by catheterization | 3.9 | 14.9 | 97 | not catheterized | subclinical | aspirin, furosemide, spironolactone, enalapril, carvedilol, diet |
CVP: central venous pressure; DILV: double inlet left ventricle; ECT: extracardiac tube; Fem: female; F: fenestration; FS: Fontan-Kreutzer surgery; HLVS: Hypoplastic left ventricle syndrome; LPB: Left pulmonary branch; NF: not fenestrated; PLE: protein-losing enteropathy; Pt: patient; SO2: arterial O2 saturation; SV: single ventricle.
Clinical presentation and initial management
Three patients had evident clinical signs of Fontan-Kreutzer system dysfunction, with generalized edema, including ascites, and one of them with disabling scrotal edema. Two patients presented with subclinical forms: patient P3 with mild lower limb edema and patient P5 with loose stools and intermittent lower limb edema. In all patients, medical treatment was insufficient for the reversal of the condition. Patients with a more severe clinical presentation required a transfusion regimen with albumin.
Four patients were catheterized prior to lymphography to evaluate Fontan system functioning. In patient P5, who only had increased alpha 1 AT clearance, without hypoalbuminemia, no prior catheterization was performed. Only in one patient with flow restriction at the interatrial level, the catheterization showed an underlying treatable hemodynamic substrate. This patient required septectomy and fenestration of the system. The rest of the patients did not require interventional or surgical procedures to optimize their condition. Central venous pressure (CVP) was elevated in all patients, with a median of 15 mmHg (range 12-19) (Table 1).
Lymphography and embolization
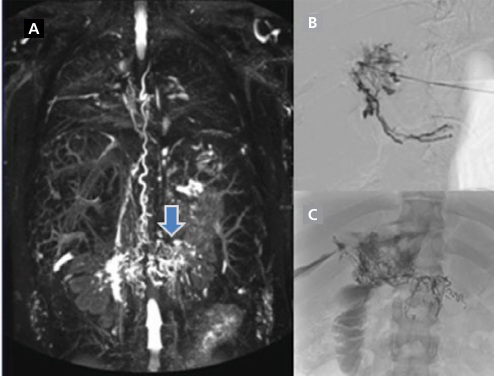
A total of 7 procedures were performed in 5 patients. In all five patients dilated and tortuous hepatoduodenal lymphatic ducts draining into the small intestine were found. In only one patient, magnetic resonance lymphography was also performed previously, and in the rest of the patients, catheterization lymphography was executed. In all patients, SHDLE was effectively accomplished (Figure 1).
Surgical technique
Catheterization lymphography is performed in the interventional room under general anesthesia. The hepatic parenchyma is accessed under ultrasound control and guidance and a 22 G gauge 10 cm Chiba needle is placed near the portal vein. It is assumed that by anatomy the lymphatic ducts are contiguous to it. Under radioscopic guidance, water-soluble iodinated contrast material is gently injected while the needle is retracted until the hepatic lymphatic ducts draining into the duodenal lumen are visualized. When the lymphatic ducts are adequately opacified, and with the needle in the hepatic parenchyma, injection of contrast material is performed to confirm how the lymphatic ducts drain a large amount of lymph volume into the intestinal lumen. Then, they are embolized by injecting 1 to 2 mL of n-butylcyanoacrylate (n-BCA) glue diluted in ethylated oil (1/6) through the same hepatic access, to seal the lymphatic branches that go from the liver to the duodenum.
Outcome
After the first embolization, all patients showed good immediate response, with an increase in albumin values in laboratory controls performed within the first ten days of the procedure. Patients P1, P3 and P5 remained with albumin values within the normal range during their evolution, until the last control, with a median follow-up of 20 months (range 12-43) (Table 2 and Figure 2).
Table 2
Results
| Pt | alpha 1 AT Cl pre procedure (mL/24 h) | Alb. pre embolization (g/dL) | Alb. at 10 days (g/dL) | Alb. at 4 months (g/dL) | Alb. at last control (g/dL) | Follow-up time (months) |
|---|---|---|---|---|---|---|
| P1 | 123 | 2.6 | 3.7 | 4.8 | 4.16 | 23 |
| P2 | 1069 | 1.8 | 2.2 | 2 | 2.3 | 39 |
| P3 | 171.3 | 2.5 | 2.69 | 4.85 | 5.12 | 43 |
| P4 | 217 | 2.2 | 2.79 | 3.17 | 3.07 | 20 |
| P5 | 272.2 | 4.04 | 4.26 | 4 | 4.2 | 12 |
Alb: albumin; Alpha 1 AT Cl: alpha 1 antitrypsin clearance; Pt: patient.
*Normal reference values: albumin: 3.2-5.3 g/dL; alpha 1 AT Cl: up to 20 mL//24 h

Patient P2 required 2 new embolizations due to failure to achieve desirable albuminemia values and persistent edema and ascites. These were performed 29 and 39 months after the first procedure, respectively. This patient did not reach normal albumin values during his evolution, but he did manage to reduce edema.
Patient P4 underwent atrial septectomy with fenestration of the system concomitant with SHDLE. At present he remains with slightly decreased serum albumin values, close to normal.
Clinically, all patients showed marked improvement in quality of life, with reduction of edema, including the patient with persistent hypoalbuminemia and the two subclinical cases, who reported improvement in self-perception of the skin and fit of their clothes.
All patients continue with the same pharmacological scheme prior to embolization, with interruption of corticosteroids at three months from the procedure.
No major intra- or periprocedural complications were observed. Regarding minor complications, 3 patients presented episode of mild self-limited melena immediately after the procedure.
DISCUSSION
Protein-losing enteropathy is a serious complication in patients with Fontan circulation. It has great impact on survival, with initially, 50% survival at five years after diagnosis. However, thanks to advances in early diagnosis and treatment in the last decade, the mortality rate has decreased significantly, and reported survival at 5 years after diagnosis is 88%, prolonging the time for the final indication of cardiac transplantation (6,7,8).
The incidence of PLE in FS described in the literature varies between 3% and 20% (6,7,8). In our case it was 5%. The pathophysiological mechanism underlying this condition is complex and multifactorial (9,10,11). In their initial series in 2017, Itkin et al. demonstrated in 8 patients that factors such as high central venous pressure, dilation and predisposing anatomy of the hepatoduodenal lymphatic connections play a crucial role in its development. These observations have led to a new approach on the importance of lymphatic circulation, offering a new paradigm for the management of this difficult-to-treat complication. Obliterating these lymphatic connections resulted in an effective reduction of protein leakage into the intestine, thus improving the patient's clinical status. (21) In our service we initiated the experience in 2019, with initially favorable results, although the number of patients treated has been limited, similar to what is observed in international cohorts.
According to the available literature, this complication can manifest itself both in the immediate post-surgical period as after many years. (9) In our series of patients, PLE presented at a median of 7 years after the performance of FS. Clinically, two patients diagnosed early showed mild or subclinical forms of the disease, while the other three had overt symptoms with severe impairment in their functional class and quality of life. The severity of hypoalbuminemia coincided with that of clinical symptoms, although no similar correlation was observed with alpha 1 AT clearance levels, and the more severe patients did not show higher levels of this protein in the stools. This could be due to a decrease in hepatic protein synthesis in the more severe cases. It is noteworthy that none of our patients presented alterations in the hepatogram during evolution. These observations underline the essential need for early detection of this complication in all patients with FS, by means of a detailed interrogation and serial analytical controls of serum albumin and alpha 1 AT in the stools.
Similary to Itkin et al. (21), and Maleux et al., (22) who have published the largest case series (with 8 and 7 patients, respectively), in our series we were also able to demonstrate, by magnetic resonance lymphography or catheterization lymphography, the presence of retrograde lymphatic flow from the liver to a dilated peri intestinal lymphatic network in the 5 patients presenting with PLE. Coincidentally with the aforementioned groups, adequate serum albumin levels were achieved in most of the treated patients after the first embolization. However, as in their case, additional procedures were sometimes necessary. In our experience one patient required two new embolizations during follow-up due to persistent hypoalbuminemia, which revealed the development of new lymphatic connections. The most serious potential complications described include progression of the material used for embolization into the hepatic artery or vein, biliary tract, systemic veins or arteries, or the pulmonary artery. In addition, portal hypertension could be expected to develop during evolution and severe local bleeding could occur. (21) None of these complications were evident in our patients. Adverse events after the procedures were all minor, mostly intestinal bleeding, manifested as mild and self-limited melena. No patient died during follow-up.
Some questions that arise in our work team from the implementation of this new treatment include:
How long will the benefits of embolization last in each patient, taking into account that the same hemodynamic conditions will be maintained over time?
When is the right time to discontinue medical treatment instituted since the diagnosis of PLE?
When is the optimal time to perform embolization, and will the earlier the procedure is performed, the better the results?
Is it necessary to implement additional routine lymphography during follow-up to evaluate persistent or newly established lymphatic connections?
When is the right time to evaluate a patient as a candidate for cardiac transplantation?
Limitations
Due to the low incidence rate of PLE in FS and the novelty of the proposed technique, the number of patients treated in our series was limited, leaving the answers to these questions unanswered.
CONCLUSIONS
Protein-losing enteropathy is a devastating complication in patients with Fontan circulation with great impact on quality of life and survival. Magnetic resonance imaging mapping and/or catheterization lymphography were key to delineate the lymphatic anatomy, lymphatic flow pattern and plan an interventional approach for embolization.
Although sample size was small, the results obtained in terms of increased serum albumin levels, clinical improvement and safety of the procedure were promising for patients with this complication. Larger scale studies will be necessary to define the long-term outcome.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web).