
Acute pericarditis is a frequent reason for consultation in clinical practice and the viral etiology is the most common in our setting. Among non-infectious causes, autoimmune and inflammatory diseases stand out, accounting for 5-15% of cases of acute or recurrent pericarditis. (1) Regarding endocrine-metabolic etiologies, the relationship between pericardial disease and hypo- thyroidism is well known, (2) but its possible association with hyperthyroidism has only been described in isolated cases such as the present one. (3)
The patient is a 72-year-old woman with hypertension and colon adenocarcinoma in remission since 2009 as the only relevant medical history, who presented to the emergency department with progressive exertional dyspnea, orthopnea, and lower extremity edema of three-week evolution. She also reported weight loss, nervousness, and tremors for the past four months, coinciding with a period of increased stress. Physical examination revealed absent vesicular murmur in the lung bases and pretibial pitting edema. On arrival, laboratory tests showed B-type natriuretic propeptide (NT-proBNP) value of 9452 pg/mL as the only finding of interest. An electrocardiogram (ECG) presented sinus rhythm with negative T waves in the right precordial leads and no other abnormalities. The transthoracic echocardiogram exhibited preserved biventricular function with moderate mitral and tricuspid regurgitation, and minimal pericardial effusion (Figure 1A). During her stay in the emergency department, she presented with palpitations, and de novo atrial fibrillation at 120 bpm, so frequency control treatment (bisoprolol 2.5 mg/24 h) and anticoagulation were initiated (Figure 1B).
After the first few days of admission, she showed good improvement in congestive signs, with resolution of symptoms and spontaneous return to sinus rhythm. An endocrinology evaluation was requested due to TSH <0.01 mU/L, for a normal value (NV) of 0.27 - 4.2 mU/L, with elevated free thiroxine and thyroid peroxidase antibodies of 5.44 ng/dL (NV 0.8 - 1.8 ng/dL) and 513 IU/ml (NV <34 IU/ml), respectively.
Further testing with thyroid-stimulating immunoglobulin antibodies, which revealed elevated levels (31.7 IU/L for a NV<1.75 IU/L), as well as scintigraphy (Figure 2A) and thyroid ultrasound, showed findings consistent with Graves-Basedow disease. The condition was interpreted as the first decompensation of heart failure in the context of hyperthyroidism, and treatment was started with oral methimazole, 10 mg every 8 hours.
Fig. 1
A. Echocardiogram with minimal pericardial effusion. B. ECG showing atrial fibrillation with controlled ventricular response.
/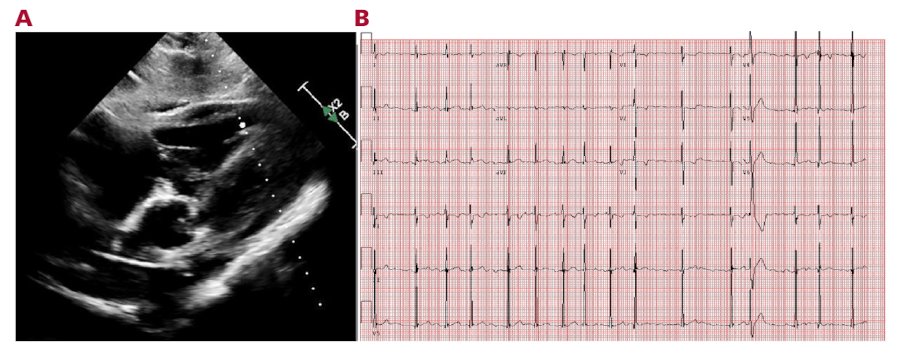
Fig. 2
A. Thyroid scintigraphy showing a thyroid gland of normal morphology, diffusely enlarged, with increased uptake and homogeneous distribution of the radiotracer, consistent with diffuse hyperfunctioning goiter. B. ECG in sinus rhythm at 70 bpm. Note the diffuse PR segment depression with inferolateral ST-segment elevation with a concave morphology, not present on previous ECGs.
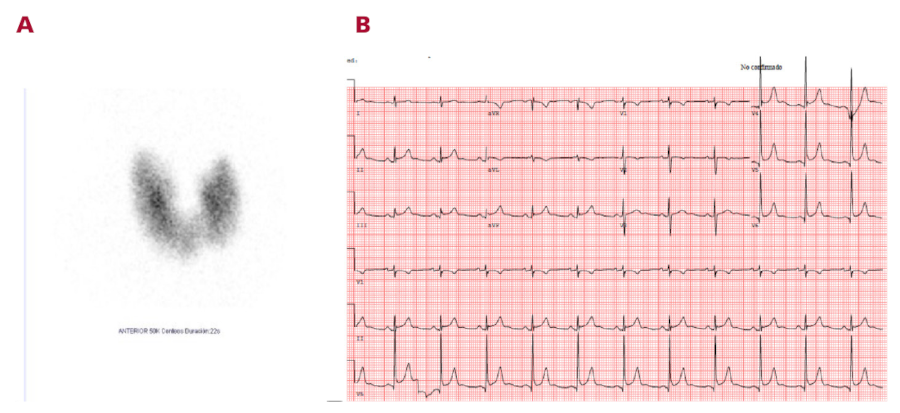
Seventy-two hours after starting antithyroid treatment, the patient presented a fever peak of 38°C and chest pain consistent with pericarditis, with pericardial friction on auscultation and ECG (Figure 2B) compatible with acute pericarditis, and no pericardial effusion on a new echocardiogram. Antinflammatory treatment was started with ibuprofen 600 mg every 8 hours and colchicine 0.5 mg daily, with rapid resolution of symptoms. In serial blood tests, inflammatory markers remained low: C-reactive protein 4 mg/L, negative PCT with normal leukocytes and negative cultures.
The patient was discharged in a state of euvolemia, with diuretic, antithyroid, and anti-inflammatory treatment initiated during hospitalization.
Graves' disease is an autoimmune thyroid disorder and the leading cause of hyperthyroidism. Its most common cardiovascular manifestations are atrial fibrillation, tachycardia, and heart failure. (1) Its relationship with acute pericarditis has been previously published by multiple authors, with cases progressing to cardiac tamponade (2) or recurrent pericarditis. (3). Although the underlying pathophysiology is unknown, some authors have proposed as a mechanism the interaction of autoantibodies with pericardial receptors, similar to what occurs in cases of ophthalmopathy and dermopathy associated with this disease. (4) Other hypotheses are based on the relationship between both entities and viral infections such as the Epstein-Barr virus, or the direct toxicity of thyrotoxicosis on the fat metabolism of the pericardium. (2) Finally, published cases of acute pericarditis after initiation of antithyroid treatment could suggest a possible direct relationship with these drugs. In our case, the temporal relationship of only 72 hours after the initiation of antithyroid treatment does not seem to point to a direct association, given that in previously published cases, the onset of symptoms is significantly later, occurring from two weeks (4) to several years later. (5)
Acute pericarditis is a common condition and is usually harmless, although in some cases it can lead to high morbidity and mortality in the absence of treatment. Graves-Basedow disease is one of the few conditions associated with pericarditis that could benefit from targeted treatment. Although the causality between the two has not yet been established, it is important to recall their association for the proper management of patients with symptoms compatible with both conditions.
Conflicts of interest
None declared. (See conflicts of interest forms on the website).
Ethical considerations
Not applicable