
Limitations of Cardiovascular Risk Scores in Primary Prevention. An Opportunity for Risk Modulators?
pp. 102-109
DOI:
https://doi.org/10.7775/rac.es.v91.i2.20609Keywords:
Risk Assessment, Plaque, Atherosclerotic, Carotid Artery Diseases, Vascular calcification, Lipoprotein(a), Primary prevention, Hydroxymethylglutaryl, CoA Reductase Inhibitors, Heart Disease Risk FactorsAbstract
Background: Cardiovascular risk scores have limitations related to calibration, discrimination, and low sensitivity. Different "risk
modulators" have been identified to improve cardiovascular risk stratification: carotid atherosclerotic plaque (CAP), coronary artery
calcium (CAC) score and lipoprotein(a) [Lp(a)].
Objectives: The aims of this study were: 1) to determine the prevalence of risk modulators mentioned in a primary prevention
population; 2) determine the concordance between the 2 methods of detecting subclinical atherosclerosis; and 3) establish which
proportion of patients should receive statins according to the initial risk stratification and after being recategorized by screening
for risk modulators.
Methods: Individuals aged 18 to 79 years who consulted for cardiovascular risk assessment and who were not receiving lipid-lowering treatment were included. The risk score was calculated in each patient using ASCVD Risk Estimator. The presence of CAP, CAC score and Lp(a) level were evaluated.
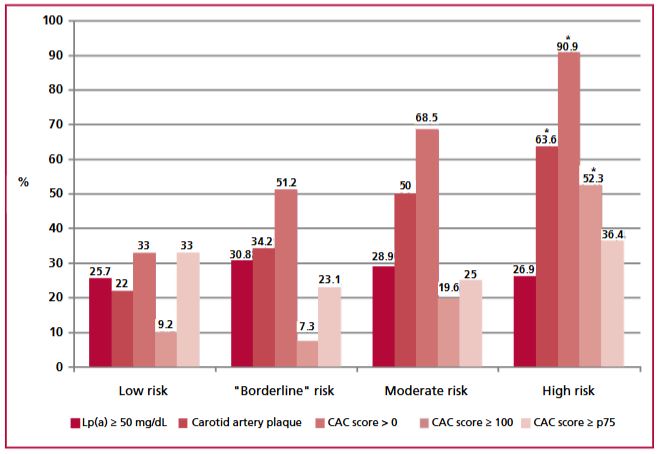
Results: The cohort was made up of 348 patients; mean age was 55.6 ± 12.2 years and 45.4% were men. In the total population,
29.8%, 36.8%, and 53.2% of patients showed Lp(a) value ≥ 50 mg/dL, CAP, or a CAC score > 0, respectively. The prevalence of CAP
and CAC score was progressively higher according to the cardiovascular risk category; however, the proportion of low-risk subjects
who had risk modulators was considerable (Lp(a) ≥ 50 mg/dl: 25.7%; CAP: 22%; CAC score > 0: 33%). In the 60 subjects <45 years ,
the prevalence of CAC score > 0 and CAP was 18.3% and 10%, respectively. The agreement between the two methods for quantifying
subclinical atheromatosis was fair (kappa= 0.33). The indication for statin treatment increased by 31.6% after evaluating the
presence of modulators.
Conclusion: The presence of risk modulators was common in this population in primary prevention, even in low-risk subjects or <
45 years. Detection of risk modulators could improve initial stratification and lead to reconsideration of statin treatment.
How to cite this article:
Siniawski DA, Masson WA, Barbagelata L. Limitations of Cardiovascular Risk Scores in Primary Prevention. An Opportunity for Risk Modulators? Rev Argent Cardiol 2023;91:102-9
https://doi.org/10.7775/rac.v91.i2.20609
Downloads
Published
Issue
Section
License
Copyright (c) 2023 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








