
Primary Outcomes and Morbi-mortality Associated Factors in the Coronary Angioplasty Argentine Registry - RAdAC
pp 461-470
DOI:
https://doi.org/10.7775/rac.es.v80.i6.1796Keywords:
Myocardial Infarction, Unstable angina, Angioplasty, Stents, Risk Factors, MortalityAbstract
Background
Percutaneous transluminal coronary angioplasty (PTCA) outcomes were compiled in the 1996 V CONAREC Registry, and in 2005, data collection was repeated using a similar methodology, giving rise to the XIV CONAREC Registry. As no general national PTCA results have been reported since, the Argentine Society of Cardiology, together with CACI, FAC and CONAREC carried out the Coronary Angioplasty Argentine Registry (RAdAC).
Objective
The aim of this Registry was to evaluate intrahospital outcome and morbi-mortality of patients submitted to PTCA according to different clinical scenarios.
Methods
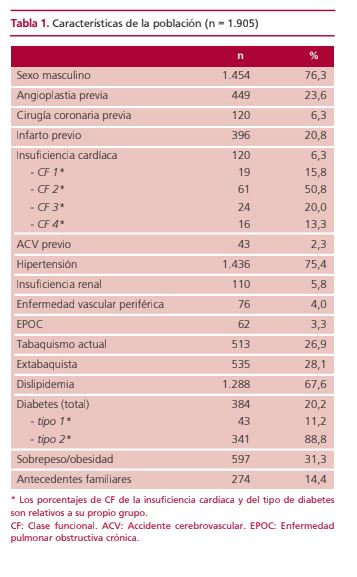
One thousand nine hundred and five patients were prospectively and consecutively included in 67 centers of Argentina during a 7-month period. Cardiovascular risk factors and clinical history were analyzed. PTCA procedures were classified as: planned, urgent or emergent and the number of affected and intended-to-treat vessels, as well as the number and type of stents implanted [bare metal (BMS) or drug-eluting stents (DES)] were estimated. Use of atherectomy, Cutting Balloon, thrombus aspiration, intravascular ultrasound (IVUS), antiplatelet drugs and intra-aortic balloon pump (IABP) was analyzed. Angiographic success was defined as residual lesion <20% and normal flow (TIMI 3).
Results
Mean age was 63.8 years. A total of 752 patients (39.5%) presented with acute myocardial infarction (AMI) and 834 patients (43.8%) with unstable angina (UA). Femoral access was used in 92.8% of the cases. Overall, 44.3% of the interventions were planned, 37.8% were urgent and 17.9% emergent.
A total of 2753 stents were implanted (1.4 per patient), 33.2% of which were DES. The primary success rate was 97% and overall mortality 1.6%: 3.2% associated to AMI, (4.3% STEMI and 1.7% non-STEMI), 0.8% to UA and 0.3% to chronic stable angina. Death-associated variables were: cardiogenic shock, need of IAPB, Killip-Kimball class 3-4, emergency PTCA, left main PTCA, ventricular function impairment, renal failure or diabetes, number of affected vessels, age and PTCA failure.
Conclusions
In our setting, most PTCAs are performed in acute coronary syndromes, almost exclusively by femoral access, with pri-
mary success comparable to that of international reports, but employing less DES. Use of Rotablator, Cutting Balloon, thrombus aspiration, IVUS and IABP implementation was lower than expected, while age, cardiogenic shock, emergency and PTCA failure were factors associated with increased morbi-mortality.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








