
Predictive Capacity of Different Surgical Risk Scores in Infective Endocarditis
pp. 408-414
DOI:
https://doi.org/10.7775/rac.es.v91.i6.20711Keywords:
Endocarditis infecciosa, Cirugía cardíaca valvular, Mortalidad, Puntuación de riesgoAbstract
Background: Infective endocarditis (IE) is a life-threatening disease that may require surgical treatment. Despite being fundamental in decision making, surgical scores were not generated specifically to stratify the risk of this disease.
Objectives: The objective of this study was to: To evaluate the predictive capacity of surgical risk scores adjusted for IE.
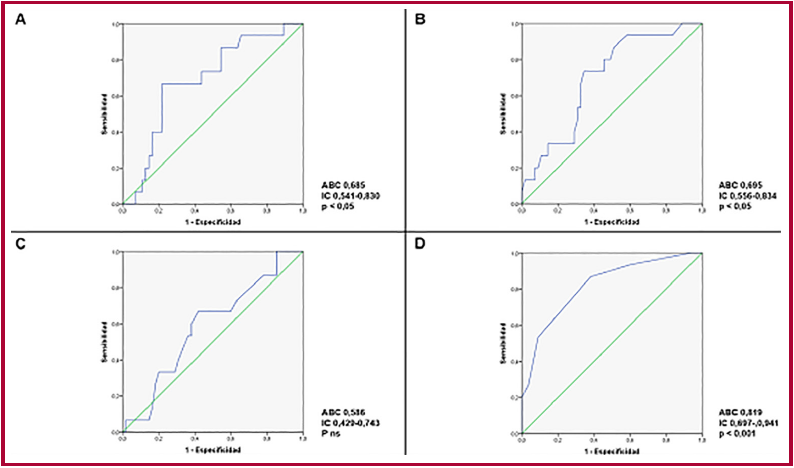
Methods: Single-center observational and retrospective study of 270 patients > 18 years, hospitalized for active IE from 06/2008 to 02/2023, of which 70 (26%) underwent central cardiac surgery. Device-associated endocarditis and patients who did not undergo cardiac surgery were excluded. The surgical risk scores analyzed were: EuroSCORE II, EURO-IE, STS-IE and PALSUSE (Prosthesis, Age >70, large cardiac destruction, Staphylococcus, Urgency, Female gender, EuroScore >10). The predictive capacity of each score was evaluated using the C statistic, calculating the area under the curve of the sensitivity/1-specificity relationship with their respective 95% confidence intervals (CI), and statistical significance.
Results: The median age (interquartile range, IQR) was 60 years (48-67) and the number of days of hospitalization were 23 (17-39). Forty-one patients (58.57%) had a prosthetic valve. Regarding the causative germs, Staphylococcus was responsible for 30% of the infections. The main indications for surgical treatment were heart failure (44%), abscess (19%) and prosthetic dysfunction (12%). Annular abscess was observed in 28.57% of patients. Urgent surgery was performed in 45.71% and emergency surgery was performed in 7.14%. Hospital mortality was 21.42%. The predictive capacity of all scores was statistically significant, except for the STS-IE. The STS-IE score presented an area under the curve (AUC) of 0.586 (95% CI 0.429-0.743). The EuroSCORE II, an AUC of 0.685 (95% CI 0.541-0.830); the EURO-IE presented an AUC of 0.695 (95% CI 0.556-0.834) and the PALSUSE an AUC of 0.819 (95% CI 0.697-0.941).
Conclusions: The results of this study suggest that the PALSUSE score was a better predictor of surgical risk in patients with active IE, compared to the Euroscore II, EURO-IE and STS-IE scores.
How to cite this article:
Ahuad Calvelo SA, Zacarías CB, Abud CM, Maidana M, Casabe H, Cortes CM, et al. Predictive Capacity of Different Surgical Risk Scores in Infective Endocarditis. Rev Argent Cardiol. 2023;91:408-414. http://dx.doi.org/10.7775/rac.v91.i6.20711
Downloads
Published
Issue
Section
License
Copyright (c) 2023 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








