
Precordial Pain with Increase of CK-MB Fraction After Excercise that Mimics Acute Myocardial Infarction: Report of 2 Cases, with Review of References
pp 337-342
DOI:
https://doi.org/10.7775/rac.v65i3.3518Keywords:
Exercise, CPK-MB, Acute myocardial infarctionAbstract
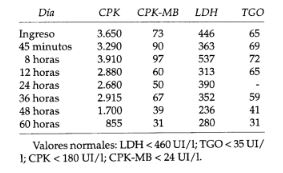
We report two male patients with precordial and epigastric pain and elevation of MB fraction of creatine kinase after exercise, which mimics acute myocardial infarction.The first patient, a 35 year-old physician consulted 48 hours after his first body-building session in 6 months. The second, a 48 year-old hypertensive habitual jogger, started 24 hours after playing a soccer game, an uncommon exercise for him. Both had increase of the MB fraction of the creatine kinase, in the second case the MB fraction of creatine kinase was 18.6% of the total creatine kinase. In both patients the result of bidimensional echocardiography was normal, without alterations in segmental wall motility. The second case also had normal stress tallium test. Because of diagnostic uncertainty, the patients underwent a coronariography which showed normal coronary arteries. We describe the reports of increase of MB fraction of creatine kinase from skeletal muscle after exercise, in subjects without myocardial pathology, and the most common sports associated with it. This elevation could be an adaptation mechanism of the skeletal muscle to the stress of training. We underline also the differences between the enzymatic patterns of skeletal muscle lesion and acute myocardial infarction: in the former, the lactid dehidrogenase increases almost immediately, the lactic dehidrogenase1/lactic dehidrogenase 2 ratio is always normal, and the creatine kinase may be elevated during several days (indeed one or two weeks); in acute myocardial infarction the lactic dehidrogenase increases after 48-72 hours, the ratio is abnormal and the creatine kinase decreases rapidly to normal values in72 hours. Neverthless, in cases with acute muscular lesion most of the patients have an increase in total MB fraction of creatine kinase (no matter which test is used), but keeping the relative index with total creatine kinase in normal values in al-most every one. Besides, the radionucleide studies are normal in the case of muscle lesion, and it could be better to use Tc99 pyrophosphate because the injured muscle can take the tracer in a total body scan. We suggest, in subjects with post-exercise pain, but without specific EKG changes and/or atypical enzymatic curve, to consider the possibility of skeletal muscle lesion and to perform the pyrophosphate scan to confirm it. Alternatively, amore cardio specific test like the troponin I could be used.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









