
Pulmonary Flow Distribution and Dynamics in Different Right Ventricle Bypass Procedures
pp 565-581
DOI:
https://doi.org/10.7775/rac.v63i6.3781Keywords:
Pulmonary flow, Bypass, Right ventricleAbstract
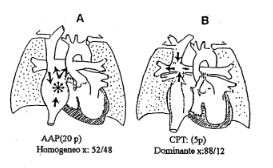
Ninety eight patients with different types of by-passing of the right ventricle procedures are evaluated as to the distribution and dynamics of pulmonary flow. A total bypass of the right ventricle had been performed in 33 and while a partial by-pass had been performed in 65 patients. Using pulmonary perfusion scintigraphy we could determine that with the present techniques of bypassing of the right ventricle, the systemic venous return is dominantly derived to the pulmonary branch were the anastomosis has been performed, both at rest and during exertion. Our results showed that total cavopulmonary connections had a relation X = 88/12%, no pulsatiles cavopulmonary shunts had X =84/16%, pulsatile cavopulmonary shunts showedX = 87/13% while partial biventricular corrections showed an X = 88/12% relationship between perfusion to both lungs. This disbalanced perfusion is due to the absence of a mixing chamber, and it explains the decreased development of the con-tralateral pulmonary branch in the no pulsatile cavopulmonary connections. This could be prevented if the competitive pulsatile flow is present. On the other hand, in atriopulmonary anastomosis, where a pulsatile mixing chamber is present, distribution of pulmonary flow is balanced and homogeneous. It is similar in both lungs during resting conditions (X = 52/48) and during exercise, beeing slightly disbalanced in the cases of cavoatriopulmonary connections (X = 68/32). In normo-functional atriopulmonary anastomosis (17/20 patients) flow in the pulmonary artery is hypopulsatile, it has slow speed, and it is trifasic anterograde as shown by transthoracic 2-D Doppler. Systolic-diastolic components are passive and show lower speed. The presystolic component is active due to the right atrial systole and shows higher velocity. In the pulmonary veins, flow is anterograde and predominantly diastolic (diastolic ventricular suction), and the right atrial systole does contribute to this flow. The diminished systolic component is due to the absence of right ventricular eyection. Patients with a total bypass of the right ventricle are unable to increase the kinetic energy (velocity of flow) during the stress of exercise, as those with a biventricular heart do. Therefore these patients cannot increase the transmitral flow as normal patients do. In the dysfunctioning atriopulmonary anastomosis (3/20 patients), flow in the inferiorvena cava is retrograde during espiration. The same is true for the pulmonary artery, while in the pulmonary veins it is only anterograde during the proto diastole, with increased flow velocity and a gradient of velocities is present when compared with the transmitral flow. This is due to left atrial restriction, or to a restrictive pattern in a patient with ventricular dysfunction. In total normofunctioning cavopulmonary connections (3/3 patients) pulmonary flow has a low velocity phasic and continuous pattern. It shows increase in velocity during inspiration with minimal acceleration in systole and diastole, while in the pulmonary veins it is bifasic and anterograde, predominantly diastolic and protosystolic. Non pulsatile partial bypass (6/65 patients) may be distinguished from the hypopulsatile (20/65 patients), the pulsatile (22/65patients) and the hyperpulsatile ones (17/65 patients) accordig to the repercusion of the competitive flow in the velocity of the flows in the superior vena cava, and the pulmonary artery branches.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









