
Previous Percutaneous Coronary Intervention Does Not Increase In hospital Mortality after Surgical revascularization: analysis of 63420 Cases
pp. 208-214
DOI:
https://doi.org/10.7775/rac.es.v81.i3.2611Keywords:
Thoracic Surgery, Myocardial Revascularization, Angioplasty, StentsAbstract
Background: Recent publications indicate higher in-hospital mortality following myocardial revascularization in patients with previous history of successful percutaneous coronary intervention. Yet, no risk models of surgical mortality have included percutaneous intervention as a risk factor.
Objectives: The purpose of this study was to analyze whether previous percutaneous coronary intervention is a risk factor of in-hospital mortality in coronary artery bypass grafting.
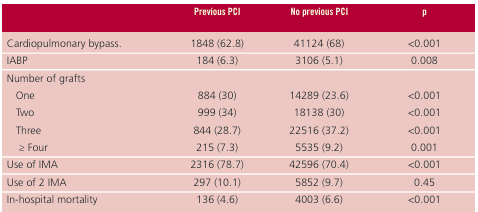
Methods: The study included 78,794 patients retrieved from the Spanish Ministry of Health database, who underwent coronary artery bypass graft surgery between January 1997 and December 2007. After applying exclusion criteria, 63,420 patients were included in the study, 2,942 (4.6%) of whom had previously undergone percutaneous coronary intervention. Continuous variables were compared using the Mann-Whitney U test or Student’s t test, and categorical variables using the chi-square test. Univariate and multivariate logistic regression analyses and a multivariate analysis including a propensity score were performed.
Results: Previous percutaneous coronary intervention was not an independent risk factor of in-hospital mortality in the multivariate logistic regression analysis (odds ratio 0.88; 95% confidence interval, 0.72-1.07; p=0.20) or after adjusting for propensity score (odds ratio 0.9; 95% confidence interval, 0.75-1.08; p=0.27).
Conclusion: Previous percutaneous coronary intervention is not an independent risk factor of in-hospital mortality in patients undergoing coronary artery bypass grafting.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








