
The Association of Antiplatelet Aggregation Effect of Aspirin and Platelet Count. Possible Dosage Implications
pp 114-120
DOI:
https://doi.org/10.7775/rac.v80i2.1901Keywords:
Aspirin, Antiplatelet Agents, Platelets, Inflammation, Interleukin 6, Myocardial RevascularizationAbstract
Background
Thirty percent of patients do not achieve an adequate antiplatelet effect despite therapy with aspirin (ASA) 100 mg/d after coronary artery bypass-graft surgery (CABGS), probably due to reduced inhibitory effect of ASA, increased platelet activation and increased platelet turnover secondary to the surgical procedure.
Objectives
To evaluate the relation between platelet count and lower antiplatelet effect and to determine if antiaggregation improves by dividing the dose of ASA.
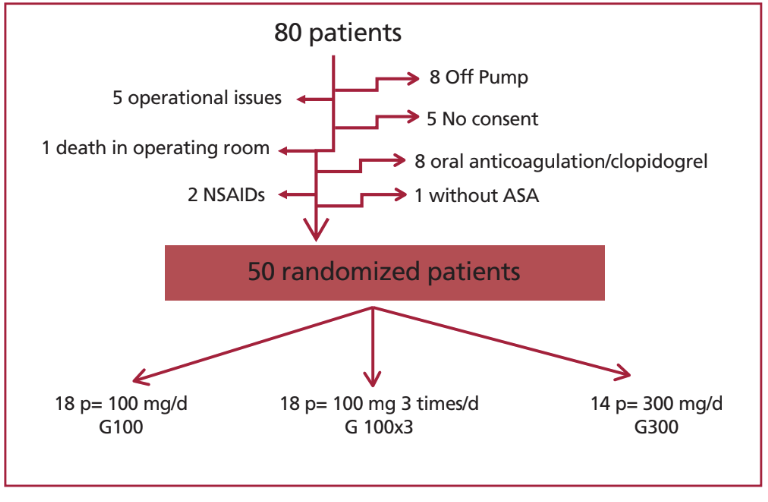
Material and Methods
A total of 50 patients undergoing CABGS (with an average of 2.95 grafts per surgery) were randomly assigned to three groups depending on the dose of ASA indicated: G100 (100 mg/d, n=18 patients), G300 (300 mg/d, n=14) and G100×3 (100 mg TID, n=18). All the patients received 100 mg/d before surgery. Platelet reactivity was assessed by whole blood impedance using arachidonic acid before surgery (T0), 24 h (T1), 72 h (T2), 7 days (T3), and one month post-CABG (T4).
Results
Before surgery, all patients had optimal values of antiaggregation (0 W). During the postoperative period, antiaggregation values were better in patients from G100×3 (p <0.05). No patients in G100×3 had values ≥6 W, which correspond to those of healthy subjects who do not receive ASA. This value was observed in 5 patients (28%) from G100 and 4 patients (29%) from G300. The association between antiaggregation and platelet turnover was statistically significant (R2=0.57; p=0.001). A daily turnover >20% was related with values of platelet aggregation ≥6 W; OR=2.1 (CI 1.8-4.21; p=0.0028).
Conclusions
In patients undergoing CABGS, the lowest antiplatelet effect of ASA was associated with the highest platelet turnover. A better antiaggregation might be achieved by dividing therapy in low dose of ASA.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








