
Cardiac Glycosides in Heart Failure With Reduced Ejection Fraction in the Era of Contemporary Guideline-Directed Medical Therapy: A Systematic Review and Meta-Analysis
pp. 32-45
DOI:
https://doi.org/10.7775/rac.es.v94.i1.20972Keywords:
Systematic review, Meta-analysis, Heart failure, Reduced ejection fraction, Cardiac glycosides -, DigitoxinAbstract
Background: Heart failure with reduced left ventricular ejection fraction remains a major clinical challenge despite widespread implementation of contemporary guideline-directed medical therapy (GDMT). Cardiac glycosides, historically used for their inotropic and neurohormonal effects, declined in use following the DIG trial (1997), which demonstrated a reduction in HF hospitalizations (HFH) with no mortality benefit. However, that trial predated modern GDMT and device therapy. The recent DIGIT-HF trial (2025) has renewed interest in this drug class by suggesting a potential benefit of digitoxin in optimally treated patients. Objective: We aimed to evaluate the impact of cardiac glycosides in patients with heart failure with reduced left ventricular ejection fraction,(≤ 40%, HFrEF) and mildly reduced ejection fraction (41%-49%, HFmrEF) receiving contemporary GDMT.
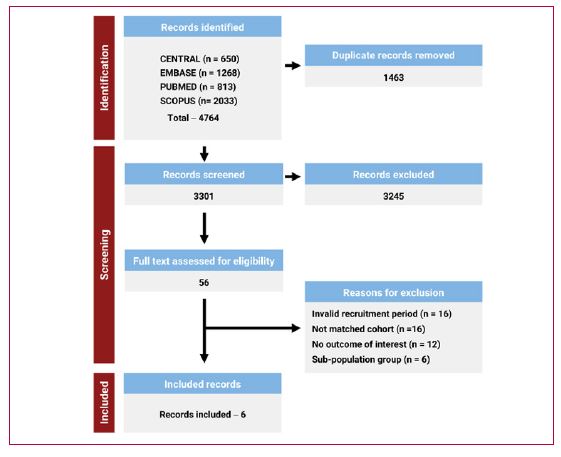
Methods: Four databases were systematically searched for randomized trials (RCTs) or propensity score-matched cohort studies recruiting adults with HFrEF and HFmrEF from the year 2000 onward, comparing cardiac glycosides with standard care or placebo and reporting at least one primary outcome (all-cause mortality or HFH). Data were pooled using an inversevariance random-effects model.
Results: Six studies met inclusion criteria: one RCT (DIGIT-HF) and five propensity score-matched observational cohorts (2000-2023) studies, comprising around 4500 cardiac glycoside users and 5500 controls. DIGIT-HF evaluated digitoxin whereas the remaining studies assessed digoxin. Pooled analysis demonstrated no significant difference in all-cause mortality (HR 1.01 [95% CI 0.67-1.53]; I² = 77%). Cardiac glycosides were associated with a significant reduction in HFH (HR 0.84 [95% CI 0.76-0.93]; I² = 0%). No significant effect was observed for all-cause hospitalizations (HR 0.95 [95% CI 0.83-1.10]; I² = 53%).
Conclusion: In the post-2000 era, cardiac glycosides may confer clinical benefit by reducing HFH in patients with LVEF < 50% receiving contemporary GDMT. However, interpretation of mortality outcomes is limited by substantial heterogeneity. This study underscores the crucial need for contemporary RCTs to clarify the role of cardiac glycosides as adjunctive therapy in contemporary management of these patients
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








