
Homografts in Pulmonar Position: Complications a Year After Surgery
pp. 457-462
DOI:
https://doi.org/10.7775/rac.v70i6.3553Keywords:
homografts, complications, evolution, anastomosesAbstract
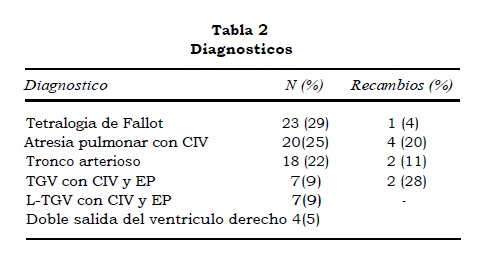
The purpose of this report was to evaluate the results of homografts between the right ventricle and the pulmonary artery, during the first year after operation. Seventy-nine consecutive patients aged 22 days to 292 months with homografts inserted in a subpulmonary position between 1991 and 2001, followed up for at least 12 months were included in the study. The median length of the follow-up was 40 months(14-124 months). The operated congenital heart lesions were: Fallot' stetralogy, 29%; pulmonar atresia and VSD, 25%; truncus arteriosus, 22%; transposition of the great arteries with VSD and pulmonary stenosis, 9%; L-TGA with VSD and PS, 9%; double outlet right ventricle, 5%. The median weight at operation was 15 kg (1,5-56 kg). The size of the homograft ranged between 9 and 26mm, mean = 19 mm. A pulmonary homograft was placed in 51% (n = 40) of the patients andan aortic homograft in the remaining 49% (n =39). In 11% (n=9), a change of homograft was needed between 15 and 122 months, mean = 61months after insertion, without operative mortality. It became obstructed in 8 patients who had a right ventricular systolic pressure over 75% of systemic level and an aneurysmal dilation was documented in one. An interventional procedure was performed in14 patients to reduce a systolic gradient. An episode of infective endocarditis was success-fully treated in 1 patient.
Conclusions:
1) The mid-term results of homografts between right ventricle and pulmonary artery were very good; 2) 11% needed a homograft replacement five years after; 3) the change of homograft was a very low risk procedure and4)failure of the homograft was dueto obstruction at the proximal right ventricular insertion or at the distal anastomoses to the pulmonary artery.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








