
Cardiovascular Risk Assessment in Primary Prevention in Patients with Type 2 Diabetes: Comparison of Multiple Scores and Detection of Subclinical Atheromatosis
pp. 198-207
DOI:
https://doi.org/10.7775/rac.es.v93.i3.20899Keywords:
Diabetes mellitus , Cardiovascular risk , Cardiovascular risk factors , Atherosclerosis , Carotid artery disease , Data correlationAbstract
Background: Risk stratification in type 2 diabetes mellitus (DM2) patients constitutes a real clinical challenge.
Objectives: 1) To stratify cardiovascular risk in a population with DM2 in primary prevention, using different risk scores; 2) To describe the prevalence of atherosclerotic carotid plaque (ACP); 3) To analyze the correlation and concordance between the different risk scores; and 4) To evaluate the discriminative capacity of the different scores to identify the presence or absence of ACP.
Methods: Observational, cross-sectional, multicenter study. Patients with DM2 in primary prevention without lipid-lowering treatment were included. The following risk scores were calculated: Framingham scores for cardiovascular disease (FrCVD) and for coronary heart disease (FrCHD), the 2018 ACC/AHA (AHA2018), PREVENT (AHA2023) and Diabetes-2 (S2-DBT) scores, and UKPDS scores for fatal coronary heart disease (UKPDS-FCHD), non-fatal coronary heart disease (UKPDS-NFCHD), fatal stroke (UKPDS-FS) and non-fatal stroke (UKPDS-NFS). Correlation and concordance between them were evaluated. the discriminative capacity of the different scores for PAC prediction analyzed using ROC curves.
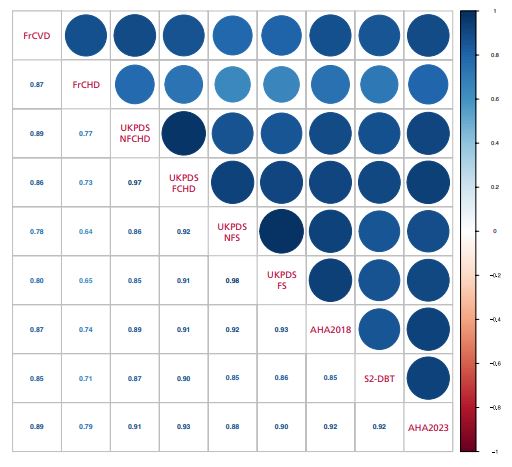
Results: A total of 170 patients were included in the study, (mean age of 61.2±10.8 years, 58.8% men). The proportion of patients classified as at least high risk was 71.2%, 39.9%, 43.6%, 23.9%, 20.9%, 53.4%, 9.8% and 49.7% when the FrCVD, FrCHD, UKPDS-NFCHD, UKPDS-FCHD, UKPDS-NFS, AHA2018, AHA2023S and 2-DBT scores, respectively, were applied. No patient was classified with risk ≥20 % when using UKPDS-FS score. A good correlation was observed between all scores assessed (Spearman´s rho values between 0.64 and 0.98). The overall agreement between the scores was fair (Fleiss Kappa coefficient of 0.38). The prevalence of ACP was 50.6%, higher in the upper risk strata of all the scores evaluated. The analysis of the ROC curves showed a very good predictive capacity of all the scores for ACP detection.
Conclusion: Cardiovascular risk was considerable for most of the scores evaluated, with an adequate correlation, but a fair concordance between the different scores. A very good predictive ability of all scores for ACP detection was observed.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








