
Percutaneous Left Atrial Appendage Closure for Thromboembolic Prevention in Atrial Fibrillation
pp. 512-518
DOI:
https://doi.org/10.7775/rac.v83.i6.7272Keywords:
Atrial Fibrillation, Atrial Appendage, Stroke/prevention and controlAbstract
Background: Atrial fibrillation (AF) produces a five-fold increase in the risk of stroke, and the exclusion of the left atrial appendage (LAA), the main source of thrombi, is an interesting therapeutic option in patients with contraindication for oral anticoagulation.
Objectives: The goal of this study was to evaluate the initial experience, immediate results and outcome at 45 days of percutaneous closure of the LAA in patients with AF and high risk of thromboembolic events, in whom chronic oral anticoagulation was contraindicated.
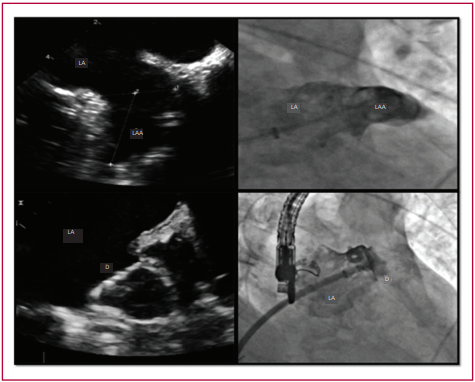
Methods: Twenty-two patients with non-valvular AF and a CHA₂DS₂-VASc ≥2 in whom there was contraindication or impossibility of long-term oral anticoagulation underwent percutaneous closure of the LAA with the WATCHMAN™ device. The patients were evaluated 45 days after the procedure by clinical assessment and transesophageal echocardiography.
Results: The implant was successful in 21 of 22 patients (95.4%). Median (interquartile range) age and CHA₂DS₂-VASc and HAS-BLED scores were 76 years (IQR 14.5), 5 (IQR 1.5) and 4 (IQR 1), respectively. Three (13.6%) periprocedural complications were observed: one cardiac tamponade requiring surgery, one concealed major bleeding and one pseudoaneurysm of the femoral artery. No device-related complications or thromboembolic events were observed during the 45-day follow-up. The LAA was adequately excluded in 95% of the cases.
Conclusions: In our initial experience, the procedure is feasible, with an acceptable risk, and can be considered a therapeutic option in patients with AF and high thromboembolic risk who cannot receive oral anticoagulation.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








