
Usefulness of Verapamil for the Electrocardiographic Indentification of AV Accessory Pathway Location
pp 211-217
DOI:
https://doi.org/10.7775/rac.v68i2.3108Keywords:
Verapamil, Radiofrequency ablation, AV accessory pathway, Wolff-Parkinson-White syndromeAbstract
Background
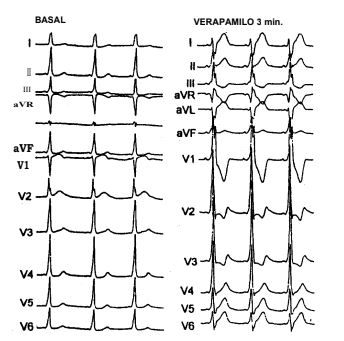
Ventricular depolarisation in the Wolff-Parkinson-White syndrome depends on two activation waves propagating simultaneously through an AV accessory pathway (AP) and the normal AV conduction system. Thus, the relative amount of ventricular mass that is depolarised from these two activation fronts may vary considerably form case to case. The electrocardiographic criteria for the diagnosis of the anatomic location of AP are based on ventricular complexes having a high degree of pre-excitation,in which all or most of ventricular activation occurs via the AP. However, when a great amount of ventricular activation depends on the impulse propagating by the AV normal conduction system, the electrocardiogrpahic diagnosis of AP location may be difficult or even equivocal.
Objectives
The main aim of the study was to determine whether verapamil, a drug known to depress impulse propagation by the AV but not within the AP node, facilitates the electrocardiographic identification of AP location.MethodsIn a whole population of 42 patients with the Wolff-Parkinson-White syndrome (27 man and 15 women, aged 12 to 52 years) 12 simultaneous ECG lead re-cordings were obtained both at baseline as well as after IV verapamil (10 mg. in 60 sec.). The diagnosis of AP location at baseline and during the peak effect of verapamil was done according to Fitzpatrick et al. criteria and compared by a chi square test.
Results
Patients were divided in two groups according to the QRS duration at baseline: Group I, with QRS> 130 m sec. (17 patients) and Group II, with QRS <_120 m sec. (25 patients). During the peak effect of verapamil the diagnosis of AP anatomic location was modified in 2 Group I patients (11.7%; p: ns)and in 12 Group II patients (48%; p < 0.05). The correct electrocardiographic diagnosis obtained in every case after verapamil administration was confirmed in every patient either by radiofrequency ablation of the AP (36 patients) or by the endocardial mapping during the electrophysiological study (6 patients).
Conclusion
Intravenous verapamil is a simple and useful tool for a reliable electrocardiographic identification of the anatomic location of AP in patients with the Wolff-Parkinson-White syndrome, particularly in those showing a small degree of ventricular pre-excitation.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









