
Characterization of Acute Myocardial Infarction Complicating the Evolution of Unstable Angina
pp 153-164
DOI:
https://doi.org/10.7775/rac.v64i2.3377Keywords:
Unstable angina, Acute myocardial infarction, Non Q wave myocardial infarction, Refractory anginaAbstract
Background
Acute myocardial infarction occurring in the evolution of unstable angina has not been completely characterized.
Objectives
1) Determine the prevalence and outcome of acute myocardial infarction complicating the evolution of unstable angina. 2) Evaluate the existence of potential risk markers of infarction in unstable angina and 3) Analyze the features of infarction, in particular the differences between Q-wave and non Q-wave infarction.
Methods
1022 patients admitted to the Enalapril en la Angina Inestable (ENAI) trial were considered. Acute myocardial infarction occurring in the evolution of unstable angina was defined when at least two oft he following criteria were present: prolonged chest pain, twofold increase above normal in CK levels and presence of new pathologic Q waves. Type of infarction comprised: Q-wave and non Q-wave infarction divided in T type, ST type and without EKG changes.
Results
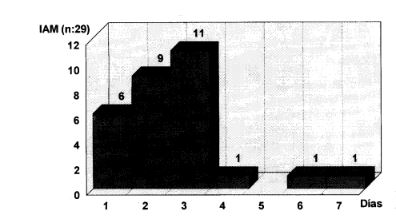
The overall incidence of acute myocardial infarction was 5% but 2% of cases were ruled out because they were considered infarctions at admission. Thus, 29 patients (3%) remained for analysis (mean age 59 ± 12 years, 24 male). Ninety percent of infarctions occurred within the first 3 days of evolution of unstable angina (21%, 31% and 38% in the first, second and third days respectively). Variables associated to complicating infarction were: 1) at admission: higher CK levels (24 ± 43 vs12 ±37; p = 0.05), unresponsiveness to nitrates, odds ratio 3.8 (1.4-11), EKG changes, odds ratio 4.1 (1-28) and new onset angina, odds ratio 4 (1.2-17);2)during CCU stay: recurrent angina, odds ratio 3 (1.3-6.7),refractory angina, odds ratio 4 (1.5-11) and EKG changes, odds ratio 4(1.6-8.6).Independent predictive variables for infarction (at admission and during CCU stay) in the multivariate analysis were: new onset angina, EKG changes and refractory angina. Absence of ST-T changes evidenced a negative predictive value for infarction of 99.2%. Excluding patients submitted to coronary surgery, mortality was 10% in infarct patients in contrast to1.3% in non infarct patients, odds ratio 9(1.8-36).The distribution of patients according to type of infarction was: 17 patients Q-wave infarction, 1patient with left bundle branch block, 11 patients non Q-wave infarction (2 cases with ST segment depression, 6 cases with T wave inversion and 3 patients without EKG changes). Non-Q wave infarction was associated to fewer episodes of angina in the previous 24 Hs., higher CK levels at admission, prior infarction and previous treatment with beta-blockers.
Conclusions
1) Acute myocardial infarction is an early event in the evolution of unstable angina, related to both a poor response to medical treatment and the presence of initial EKG changes in unstable angina. 2) Acute myocardial infarction significantly increases the risk of death in unstable angina, irrespective of revascularization procedures. 3) Unstable angina without EKG changes identifies a subgroup of low risk for infarction. 4) A high proportion of infarctions complicating unstable angina was of the non Q-wave type that were associated to previous coronary artery disease manifestations.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









