
De novo Atrial Fibrillation in ST-Elevation Acute Myocardial Infarction. Analysis of the ARGEN-IAM-ST Registry
pp. 97-104
DOI:
https://doi.org/10.7775/rac.es.v93.i2.20876Keywords:
Atrial Fibrillation, ST-segment elevation myocardial infarctionAbstract
Background: Atrial fibrillation (AF) is the most frequent arrhythmic complication in patients with acute coronary syndrome (ACS), and its incidence ranges between 2.3 % and 21 %.
Objective: To determine the incidence and predictors of de novo AF in patients with ST-segment elevation myocardial infarction (STEMI).
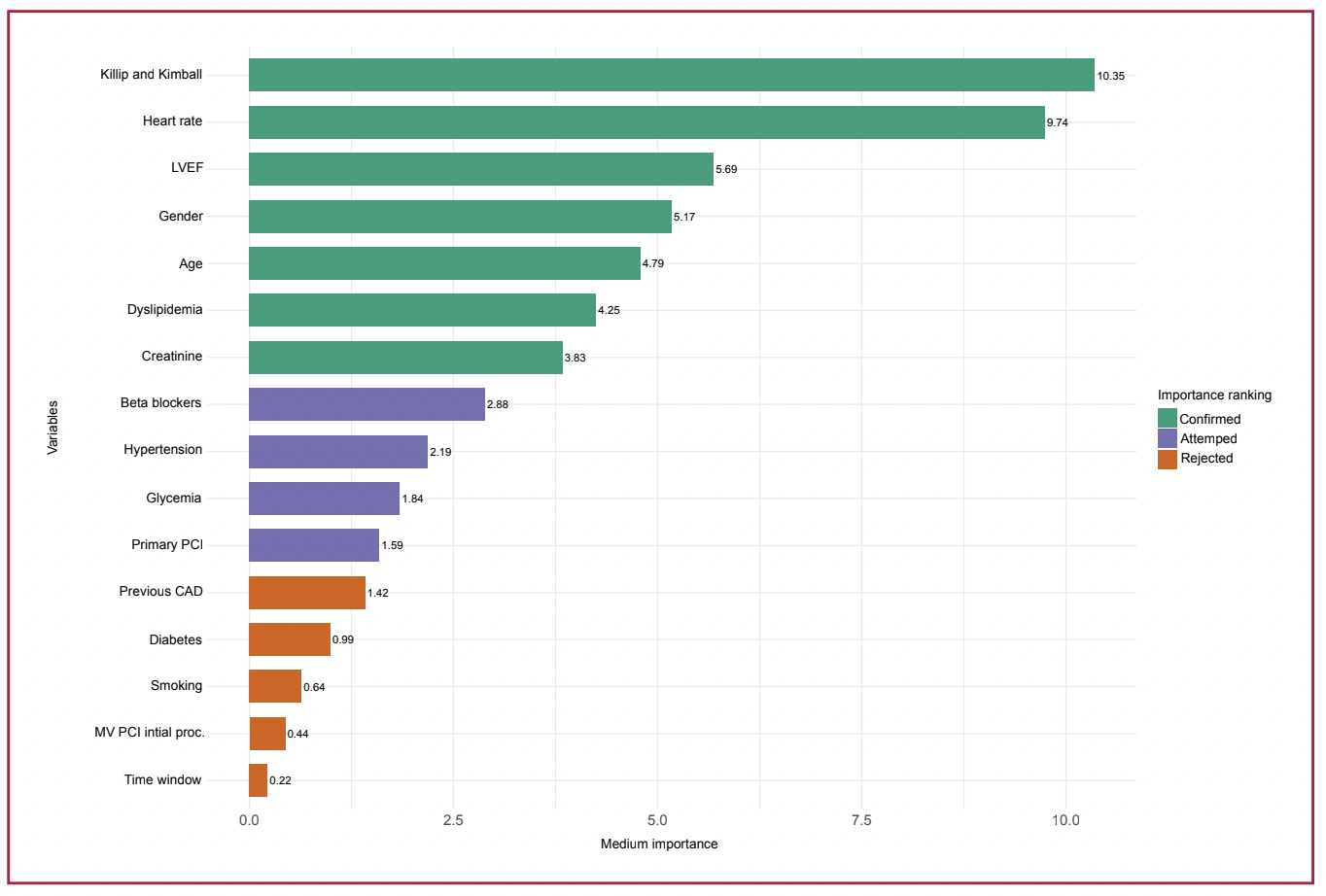
Methods: The database of the ARGEN-IAM-ST continuous registry was analyzed. Conventional descriptive statistics were used. To reduce dimensionality and identify those variables associated with the outcome of interest, Machine Learning algorithms were used, and a multivariate logistic regression analysis was performed to identify those factors associated with de novo AF. These were included in a final ranking model which was assessed by using the receiver operating characteristic (ROC) curve. A p-value <0.05 was considered statistically significant.
Results: We included 7292 patients with STEMI. A total of 4.3 % had de novo AF during hospitalization. This group was older (67 vs. 60 years, p <0.001), with higher heart rate and Killip and Kimbal score and lower left ventricular ejection fraction (LVEF) on admission. These patients had a higher incidence of stroke (2.5 % vs. 0.8 % p = 0.002) and in-hospital death (23.3 % vs. 8.2 %, p <0.001), but de novo AF was not an independent predictor of mortality. The following variables were independent predictors of in-hospital de novo AF after STEMI: stratified age (50 to 59 years: OR 2.16, 95 % CI 1.11-2.73; 60 to 69 years: OR 1.77, 95 % CI 1.07-2.96; 70 to 100 years: OR 3.98, 95 % CI 2.60-6.26), Killip and Kimball score (B: OR 1.72 95 % CI 1.19-2.46; C: OR 1.09, 95 % CI 0.31-2.91, D: OR 2.48, 95 % CI 1.60-3.78), tachycardia (OR 2.41, 95 % CI 1.74-3.31) and LVEF <35 % (OR 1.62, 95 % CI 1.74-3.31). The area under the ROC curve (AUC ROC) of the model was 0.73; the sensitivity and specificity were 77 % and 62 %, respectively.
Conclusion: De novo AF was a relatively frequent complication. Factors such as age, heart rate, hemodynamic profile on admission and ventricular function were shown to be predictors of de novo AF after a myocardial infarction during hospitalization. However, de novo AF was not independently associated with in-hospital mortality.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








