
Roundtable Cardiovascular Evidence Gaps in Adults Over 80 Years of Age
pp. 188-197
DOI:
https://doi.org/10.7775/rac.es.v93.i3.20897Keywords:
Frailty , Comprehensive cardiology assessment , Evidence gaps, Cardiovascular disease , Older adultsAbstract
Background: Current clinical practice guidelines show limitations regarding patients over 80 years of age due to their underrepresentation in clinical trials and the complex interaction between frailty, multimorbidity, polypharmacy and cardiovascular events.
Objectives: The aim of this study was to discuss existing management gaps and to establish recommendations for this population, through discussion with referring physicians in cardiology and geriatrics.
Methods: A meeting was held using structured consensus methodology in roundtables assembling 34 cardiologists and 6 geriatricians to analyze different clinical scenarios: frailty, polypharmacy, cardiovascular prevention, heart failure, atrial fibrillation and acute coronary syndromes. Management strategies were evaluated according to three categories (robust, mild frailty and moderate frailty) by structured discussion and anonymous voting. In this publication we present the results obtained in the first four scenarios.
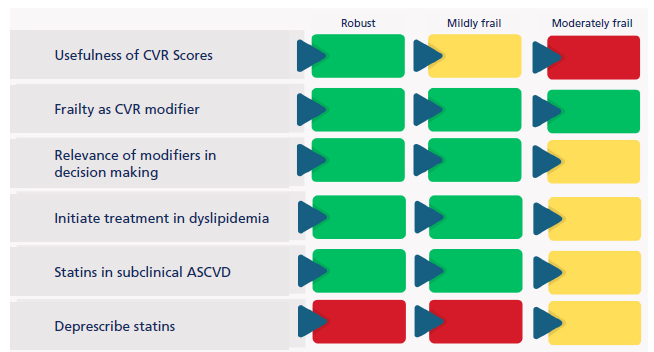
Results: An inverse association was observed between therapeutic intensity and degree of frailty. Most physicians considered it relevant to assess frailty and extracardiologic medication, and to evaluate deprescribing during follow-up. In cardiovascular prevention, acceptance of lipid-lowering treatment initiation decreased significantly with increasing frailty (82.1% in robust vs. 23%.1% in moderate frailty), whereas deprescription of statins increased (23.1% in robust vs. 41% in moderate frailty). In heart failure with preserved ejection fraction, gliflozins showed high acceptance in patients without volume overload (94.6% in robust vs. 54.1% in moderate frailty). For patients with reduced ejection fraction, initiation of quadruple therapy decreased significantly with frailty (45.9% in robust vs. 2.7% in moderate frailty), whereas maintenance of treatment in recovered ejection fraction decreased as frailty increased (91.9% in robust vs. 59.5% in moderate frailty).
Conclusions: The degree of frailty significantly influenced therapeutic decision-making in octogenarian patients, with a trend towards more conservative approaches as the degree of frailty increases. These findings suggest the need for treatment algorithms stratified by frailty and highlight the importance of incorporating comprehensive patient assessment into cardiovascular care protocols.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








